
In this guide, we go over what it takes to build a mental health chatbot that actually works in production: the layered safety architecture, the HIPAA/FDA/state-law compliance stack, the tech stack and tools, a 12-week MVP plan, and the monetization models that hold up in 2026. The focus throughout is on practical mental health chatbot development for product teams, therapist practices, and healthcare orgs that need to ship something safe, compliant, and useful.
Top Takeaways:
- A mental health chatbot is not a single feature. It is a layered system (LLM, retrieval grounding, deterministic safety policy, human handoff, audit logs), and the safety architecture is the product.
- The model that works in 2026 is hybrid care: the bot handles intake, triage, psychoeducation, and between-session continuity; licensed clinicians handle anything that needs clinical judgment.
- Compliance is a stack, not a checkbox. HIPAA when you handle ePHI, FDA/SaMD if you make clinical claims, plus state consumer health data laws, the FTC Health Breach Notification Rule, AI transparency requirements, and SOC 2 Type II for enterprise deals.
- A focused MVP (one workflow, basic escalation, minimal data retention) typically lands at $30K to $80K in 12 weeks. The three monetization paths that pay rent are B2B employee wellness, freemium plus paid human care, and reimbursement for FDA-cleared digital therapeutics (hardest path).
Table of Contents:
- What is a Mental Health Chatbot?
- How Do Mental Health Bots Work?
- Why Build a Mental Health Chatbot in 2026?
- Mental Health Chatbot Use Cases and Limitations
- Essential Features of a Safe Mental Health Chatbot
- How to Build a Mental Health Chatbot MVP in 12 Weeks
- Safety and Ethical Considerations for Mental Health Chatbots
- Regulatory Compliance Guide for Mental Health Chatbots
- Mental Health Chatbot Architecture and Tech Stack
- Best Tools and Platforms for Mental Health Chatbot Development
- Which Mental Health Chatbot Platform Should You Choose?
- Mental Health Chatbot Examples: What Product Teams Can Learn From Them
- What Does a Mental Health Chatbot Cost to Build?
- Mental Health Chatbot Monetization Models in 2026
- How to Measure Mental Health Chatbot ROI
What is a Mental Health Chatbot?
A mental health chatbot is an AI-powered conversational program that provides mental health support, psychoeducation, self-assessment, mood tracking, and structured coping exercises through text or voice. It is not a replacement for mental health professionals. It is a front-door layer that handles the repetitive, structured work and routes people to a human when the situation needs clinical judgment.
Mental health chatbots are typically used to help people manage day-to-day stress, anxiety, sleep issues, low mood, and other common mental health concerns, and to support clinics in triage, intake, and between-session continuity. They are not designed to diagnose or treat mental illness on their own, and the better products are explicit about that boundary.

The chatbot’s intelligence can be surfaced to users in several ways:
- a custom mental health mobile app
- a web portal (common for employer and clinic rollouts)
- an instant messenger integration (WhatsApp, Messenger, SMS)
- an avatar-based or voice-based experience
The form factor depends on where your users already are, what level of clinical oversight is involved, and what data you can safely handle in each channel.
How Do Mental Health Bots Work?
Most mental health chatbots run on a five-stage dialog system. In older rule-based bots each stage is a discrete component. In modern LLM-based bots several stages collapse into a single model call, but the conceptual pipeline still holds and is the easiest way to reason about where things go right or wrong.
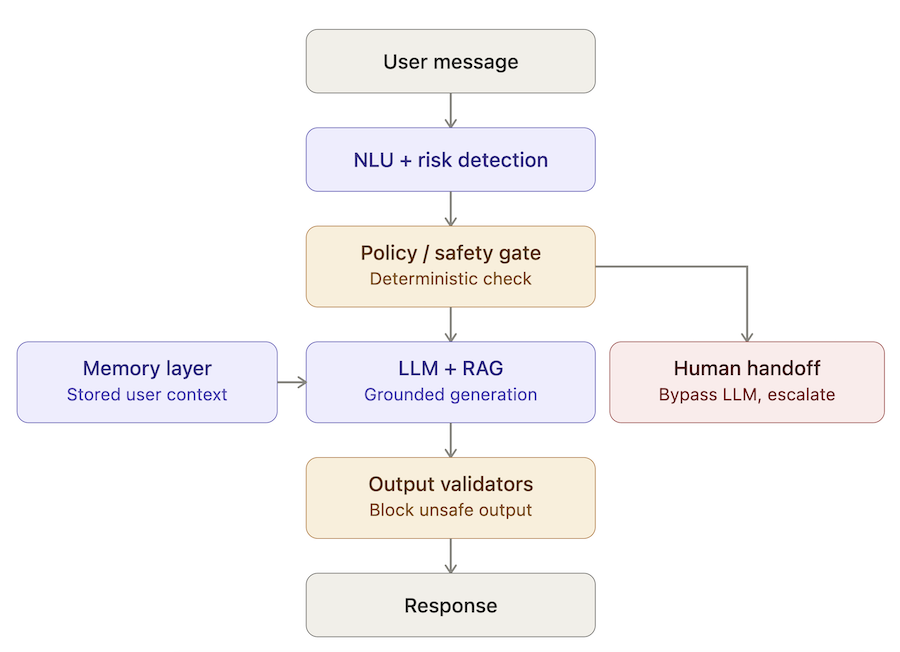
Modern mental health chatbot architecture: NLU and a deterministic safety gate sit in front of the LLM, with retrieval grounding, memory, and output validation around it. Crisis-level inputs bypass the LLM entirely.
- Speech recognition (optional)
For voice-enabled bots, off-the-shelf speech-to-text (STT) algorithms transcribe the user’s voice into text. Text-only bots skip this step.
- Natural Language Understanding (NLU)
The system processes the user’s input to extract intent (what they want), entities (specific parameters and attributes in the message), and emotional state (sentiment analysis). In a CBT-style flow, this is where the bot decides whether the user is venting, asking for a coping exercise, or showing distress signals that need an escalation. Solid NLU is what separates a chatbot that actually helps from one that produces generic chatbot’s responses.
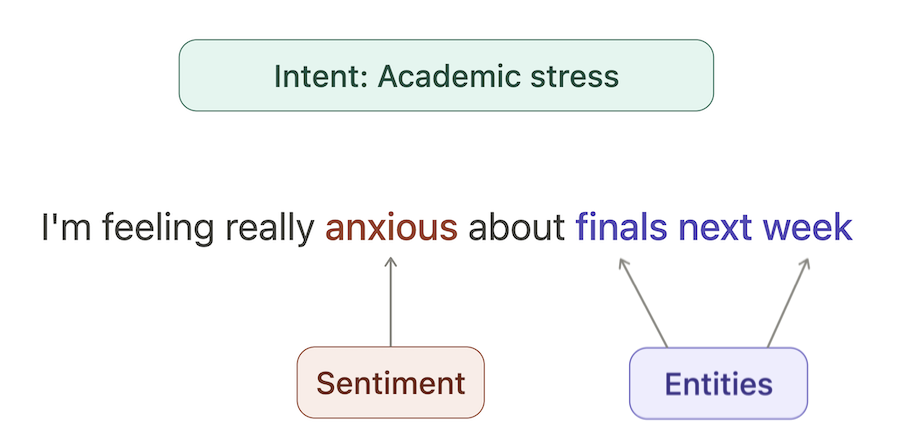
Modern NLU extracts more than just intent and entities. Sentiment and risk signals run in parallel and feed the safety gate downstream.
- Dialog and Task Manager
This module controls the flow of the conversation. It tracks context across turns (what the user said earlier, where they are in a flow, what data has been collected) and decides what should happen next: ask a follow-up, run a coping exercise, hand off to a clinician, or trigger a safety protocol. In a safety-first mental health chatbot, this layer is also where deterministic policy gates live (more on that in the Safety section).
- Natural Language Generation (NLG)
Once the dialog manager decides what to say, the NLG module produces the actual response. In rule-based systems this is a predefined template; in LLM-based systems the model generates a response constrained by prompts, retrieved context, and runtime guardrails. This is where the chatbot’s capabilities show up most visibly to the user.
- Text-to-Speech Synthesis (optional)
For voice bots, a speech synthesis module converts the generated text back into spoken audio.
The big shift in 2026 is that the LLM has absorbed a lot of the NLU and NLG work that used to require separate models. That makes prototyping faster, but it also means the dialog manager and the safety layer have to do more, not less, of the heavy lifting. We unpack that stack in detail later in this guide.
Why Build a Mental Health Chatbot in 2026?
If you run a therapist practice, sit inside a healthcare org, or are building a consumer-facing product, mental health chatbot development is no longer a “let’s experiment with AI” project. It’s a practical tool for closing access gaps, cleaning up intake, and protecting clinician time. The case for building one in 2026 comes down to six concrete shifts.
Mental Health Chatbots Help Close Access Gaps
The bottleneck in mental health support isn’t lack of demand. It’s lack of capacity. Waitlists are long, in-network options are limited, and many people give up before they ever reach a clinician. Mental health chatbots help close that gap by providing a 24/7 entry point that’s available regardless of geography, schedule, or insurance status.
Where this pays off:
- Accessibility without adding staff. A bot can provide instant information any time of day, which helps clients who work unconventional shifts, can’t find availability, or are stuck behind geographical barriers (especially where face-to-face counseling is limited).
- Lower stigma, more disclosure. Clients often feel more comfortable starting with a chatbot because of perceived anonymity, and may be more willing to disclose sensitive information early. You’ll see this pattern show up across more than one recent study.
- A real first step for people who otherwise wouldn’t take one. For many users, a chatbot is the first frictionless entry into psychological health services. Even if they eventually move to a human clinician, the bot is what got them to start.
Hybrid Care Is Becoming the Practical Model
The winning model in private practice isn’t “AI therapist.” It’s hybrid care: a therapeutic chatbot handles the repetitive front-door work, and a clinician takes over when the situation needs clinical judgment.
When clients use a chatbot to get started, they arrive at the first session less “cold” and with fewer unanswered basics. The clinician spends less time on logistics and more time on the actual problem. Done well, hybrid care also gives mental health professionals a structured way to extend support between sessions without burning evening and weekend hours.
The handoff is the load-bearing piece: the bot should collect and summarize, then route to a human therapist the moment it hits your “needs a clinician” threshold.
Read more on chatbot development cost
Chatbots Improve Intake, Triage, and Between-Session Continuity
A chatbot earns its place in a mental healthcare workflow not by replacing care, but by smoothing the operational edges around it.
- Cleaner intake. The bot can run self-assessment prompts, collect basics, and summarize what matters. Your practitioner isn’t burning 15 minutes on admin before therapy even starts.
- Better triage. With a structured front-door flow, you can route low-acuity users to self-guided resources and route higher-acuity users to a human faster, instead of treating all incoming requests the same way.
- Between-session continuity. A bot can deliver lightweight check-ins, reminders, and structured exercises so the next session starts with signal, not recap.
The pattern that works: the bot is allowed to collect, suggest, and follow up. It’s not allowed to decide on a plan of care. That line is what keeps the system safe.
Mental Health Chatbots Can Reduce Provider Burnout
The therapist shortage problem in 2026 doesn’t just show up in waitlists. It shows up in your calendar: late cancellations, repetitive admin work, and clinicians spending energy on things that don’t require their training.
Mental health chatbots can offload work in very specific ways:
- Pre-session and between-session support. A bot can deliver structured check-ins, reminders, and coping exercises, often providing positive emotional support, so the next session opens with signal rather than recap.
- Protecting clinician time for people in critical condition. If your clinicians are spending prime hours answering routine questions, you’re under-using your most expensive resource. A bot can handle the FAQ layer and basic triage.
- Operational savings. For clients: less travel, fewer phone calls, fewer reschedules. For your practice: fewer wasted slots, fewer repetitive admin minutes, and better utilization without extending clinical hours.
The goal here is not “turn software into mental health advisors.” The goal is to give clients a reliable first step and let clinicians stay clinicians.
Where the ROI Comes From
If you’re trying to justify a mental health chatbot internally (or externally to a buyer), the ROI story is rarely “we replaced X clinicians.” It’s a stack of smaller, measurable wins that add up.
Typical ROI levers:
- Reduced admin time per client.
- Improved engagement and retention (lower drop-off in the first 2 to 4 weeks of care).
- Fewer no-shows and late cancellations through structured reminders and pre-session prep.
- Increased throughput without extending clinical hours.
- Lower per-user support cost on routine FAQ-level questions.
- Stronger employer or payer outcomes data when the bot is part of a measured program.
For B2B buyers (employers, payers, health systems), the ROI conversation is increasingly about access metrics and engagement, not just cost per session. For consumer products, ROI is about retention and conversion from free chat into paid care.
What the Evidence Actually Supports
The honest framing in 2026 is “promising, not magical.” The clinical signal is real but modest, and most of the well-supported outcomes come from structured, time-limited interventions paired with clear escalation and human oversight.
What the evidence supports today:
- Modest, measurable improvements in symptoms of depression and anxiety from structured CBT-style chatbots, especially in short-term studies (2 to 8 weeks).
- Reductions in feelings of isolation and improvements in disclosure when the chatbot is positioned as a low-pressure first step.
- Higher engagement than information-only controls in several randomized trials, particularly with younger users and university populations.
- Healthcare professionals increasingly view chatbots as potentially helpful for mental care when paired with clinician oversight (see this recent survey).
What the evidence does not support:
- Replacing licensed mental health professionals.
- Treating acute mental illness or severe symptoms without clinical involvement.
- Long-term outcomes claims from short-term studies. The data isn’t there yet, and any product that claims it is misreading its own evidence.
Related: Machine Learning App Development Guide
Mental Health Chatbot Use Cases and Limitations
A mental health chatbot can do a lot of useful work, but only if you’re honest about where it belongs and where it doesn’t. The strongest products are narrow on purpose: they pick a small number of high-value use cases, build them carefully with clinical input, and refuse to drift outside those boundaries. The weakest products try to be a general-purpose AI therapist and end up generating the kind of advice that gets a company on the front page for the wrong reasons.
Below are the use cases that actually work in production, plus a clear line on where mental health chatbots should not be used.
Daily Emotional Check-Ins and Mood Tracking
One of the most reliable use cases is the simplest: a daily or weekly check-in that asks the user how they’re doing, captures a mood score, and surfaces patterns over time. This is low-risk, high-engagement work that people genuinely come back to.
What this looks like in practice:
- A short structured prompt (mood, energy, sleep, stress) instead of an open “how are you” prompt that produces messy free text.
- Mood tracking visualizations the user can review weekly or monthly.
- Lightweight nudges when the bot detects a downward trend, without making clinical claims.
The trap to avoid: turning a check-in into a diagnosis engine. The chatbot’s responses should reflect, validate, and surface trends, not label conditions. If a pattern looks concerning, the right response is “would you like to talk to someone about this,” not a list of possible disorders.
Guided CBT, Mindfulness, and Coping Exercises
Structured, time-limited interventions are where mental health chatbots have the strongest evidence base. CBT-style flows, mindfulness exercises, grounding techniques, and short coping protocols all translate well to a chat interface because they’re already structured, scripted, and skill-based.
Examples that work well:
- Thought reframing exercises (identify the thought, evaluate the evidence, generate a balanced alternative).
- Grounding exercises for moments of acute anxiety (5-4-3-2-1 senses, paced breathing).
- Short mindfulness prompts users can run in 2 to 5 minutes.
- Sleep hygiene protocols and behavioral activation plans.
The product principle here: a chatbot is a great delivery mechanism for content a clinician would already trust. It’s a poor mechanism for inventing new clinical content on the fly.
Intake, Triage, and Routing to Human Support
If you’re building inside a clinic, healthcare org, or B2B platform, intake and triage is often the highest-ROI use case. The bot collects basic information, runs a structured screen, and routes the user to the right next step: self-guided resources, an appointment with a clinician, or a higher-acuity escalation.
Why this works:
- It saves clinical time at exactly the point where clinicians don’t add value (admin and basic screening).
- It makes the first appointment more productive because the clinician walks in with structured context, not a blank slate.
- It surfaces high-risk users earlier than a manual intake queue would.
The bot’s job is to collect and summarize, not to decide. Routing rules should live in deterministic logic, reviewed and signed off by clinical leadership, not in an LLM’s free-form judgment.
Between-Session Support for Clinics and Therapy Practices
Therapy works best when there’s continuity between sessions, but most clinicians don’t have the bandwidth to provide that continuity manually. A chatbot can fill the gap with structured between-session support, while keeping the human therapist in the loop.
What this looks like:
- Homework reminders and check-ins on assigned exercises.
- Mood and symptom tracking that feeds into the next session as a clinical summary.
- Crisis-aware nudges that escalate to the clinician (or to crisis resources) when patterns shift.
- Lightweight psychoeducation aligned with what the clinician already covered.
The key design rule: the clinician must be able to see what the bot has been doing with their client, and the bot must never contradict or undermine the clinician’s plan of care.
Employee Wellness and Student Mental Health Support
Two B2B contexts where mental health chatbots have proven especially useful are employee wellness programs and student mental health services in universities. Both populations share a common pattern: large user base, limited clinical capacity, real demand for low-friction support, and a clear procurement path.
What works in these settings:
- Anonymous or pseudonymous access (employees and students are often hesitant to use named services).
- Skill-based modules tied to common life stressors (work pressure, exams, sleep, relationships).
- Clear escalation to in-network EAP providers or campus counseling services.
- Aggregate (de-identified) reporting for the program owner, never individual-level disclosures to employers or universities.
Where teams trip up: assuming employer or university buyers will tolerate weak privacy guarantees because the buyer pays the bill. They won’t, and they shouldn’t. The end user’s trust is what makes these programs work.
Where Mental Health Chatbots Should Not Be Used
The list of things a mental health chatbot should not do is shorter than the list of things it can do, but it matters more.
Hard “no” categories:
- Diagnosing mental illness or any mental health disorders. The bot can reflect, validate, and route. It cannot label.
- Recommending or adjusting medication. Any medication-related question should route to a clinician, full stop.
- Acting as the sole source of support for someone in acute crisis. Crisis flows must escalate to a human (or to crisis resources). A bot is not a clinician on call.
- Replacing therapy for severe or complex mental health disorders. Bots are useful adjuncts for many people, but they are not a substitute for treatment of severe depression, suicidality, psychosis, or trauma.
- Pretending to be human. Users should know they’re talking to AI. Pretending otherwise is both an ethical failure and, in a growing number of jurisdictions, a regulatory one.
A useful gut-check before you ship: if a clinician would not feel comfortable defending a specific bot behavior in a case review, that behavior should not be in production.
Essential Features of a Safe Mental Health Chatbot
Once you know what the bot is for, the next question is what it actually has to contain. The list below is the minimum feature set, the key features, for a mental health chatbot you’d be willing to ship, audit, and put in front of vulnerable users. Skip any of these and you’re building a demo, not a product.
Every feature here exists in service of two goals: keep users safe, and keep your team’s name off the front page.
Clear Role, Boundaries, and User Disclaimers
Users should know exactly what your chatbot is, what it isn’t, and what it won’t do, in plain language and at the moments where it matters.
Where to put disclaimers:
- On first launch: what the bot does, what it doesn’t do, what to do in an emergency.
- Before sensitive flows (mood check-ins, crisis-related topics, anything that could be mistaken for clinical advice).
- In the bot’s persistent identity: the bot identifies itself as AI, every time. No “I’m your therapist” cosplay.
Practical principles:
- Plain English, not legal poetry. Users should understand the disclaimer in five seconds.
- Decisions where it counts. A disclaimer in the footer of a settings page is not a disclaimer.
- Consistent voice. The bot should redirect to professional help the same way every time, not improvise based on phrasing.
Crisis Detection and Escalation Logic
Crisis detection is the feature that separates a wellness chatbot from a liability. It’s not “the bot says something empathetic.” It’s a deterministic workflow that runs on every message, before any LLM response is generated.
What this looks like in product terms:
- Real-time risk signals on every turn: keyword and intent patterns, simple severity scoring, sentiment cues.
- Coverage for indirect or “coded” expressions of distress, not just obvious phrases.
- A clear escalation threshold that triggers a different response mode, not “more empathetic” replies.
- Hard-coded crisis resources that surface immediately when escalation triggers (no model debate, no follow-up questions).
The deeper architecture (policy gates, response modes, deterministic overrides) is covered in §7 Safety. From a product feature perspective, what matters is that crisis detection is always on, runs before the LLM speaks, and is auditable after the fact.
Human Handoff to Therapists or Support Teams
A chatbot without a real handoff path is a closed loop. The handoff is what keeps the bot useful instead of dangerous.
What “real” looks like:
- For practice-owned bots: the handoff routes to a live clinician, an on-call workflow, or a warm transfer to your support channel.
- For B2B and consumer bots: the handoff routes to crisis resources, an in-network EAP provider, or a structured callback flow with explicit timing expectations.
- Always: the bot tells the user clearly what just happened (“I’m connecting you to a person”) and what to expect next.
Anti-patterns to avoid:
- Bargaining loops (“are you sure you want to talk to someone?”). No.
- Quiet handoffs the user doesn’t understand. They should know a human is now involved.
- Handoff paths that work in office hours and silently break at 2 AM. Define your after-hours behavior, including emergency resources.
Consent, Privacy, and Data Retention Controls
Mental health data is among the most sensitive categories you can handle, and users notice when a product treats it casually. Consent and data controls aren’t a compliance afterthought; they’re a core product feature.
What to build:
- Explicit, specific consent: what you collect, how it’s used, who can see it, how to revoke.
- Granular retention controls: separate retention rules for transcripts, mood data, journal entries, and aggregate analytics.
- User-facing data tools: export your data, delete your data, reset memory, end your session.
- A clear distinction between “product preference memory” (low sensitivity) and clinical content (high sensitivity), with different controls for each.
The compliance scaffolding behind these features (HIPAA, state consumer health data laws, the FTC Health Breach Notification Rule) is covered in §8 Regulatory Compliance.
Mood Tracking, Journaling, and Guided Exercises
These are the day-to-day features that make a mental health chatbot useful between crises, and they’re often the reason users come back. Done well, they reinforce healthy patterns and feed clinical context back to a clinician (when there is one).
Core capabilities:
- Structured mood and symptom tracking with simple visualizations (weekly, monthly trends).
- Lightweight journaling with optional AI-assisted reflection prompts. Reflection, not interpretation.
- A library of guided exercises (CBT-style reframes, grounding, paced breathing, sleep protocols) the user can run in 2 to 10 minutes.
- Personalized reminders and streaks, used carefully, with no manipulative engagement loops.
The product line to hold: helpful structure, never dependency. A mental health chatbot should make users more capable, not more attached to the app.
Admin Dashboard, Analytics, and Clinical Review Tools
The features above are user-facing. The features in this section are operator-facing, and they’re what turn a chatbot from “shipped” into “operable.”
What admin tooling needs to do:
- Conversation review with strong access controls (least-privilege, audit-logged, retention-limited).
- Safety incident dashboards: every escalation event with timestamps, triggers, and outcomes.
- Content management: update guided exercises, prompts, and crisis resources without redeploying code.
- Clinical oversight workflows: a defined cadence for clinician review, edge-case triage, and content sign-off.
- Aggregate, de-identified analytics for product owners and B2B buyers, with strict guardrails against re-identification.
If you can’t answer “who reviewed this conversation, when, and why” in under a minute, your admin tooling isn’t ready. This is the part of the product that buyers, regulators, and your own clinicians will all evaluate first, in that order.
How to Build a Mental Health Chatbot MVP in 12 Weeks
This is the practical, no-magic, step-by-step guide to mental health chatbot development. Twelve weeks, clear deliverables each week, a safety-first posture, and enough structure to keep you from shipping a clever demo that falls apart the first time a real user types something messy.
One note up front: if you’re touching anything that looks like PHI, treat privacy and security as a build constraint, not a “week 12 task.”
Weeks 1-2: Define Scope, Risk Boundaries, and Success Metrics
- Goal: Decide what the bot is, and what it isn’t, before you write a single prompt.
- Cover: Primary use cases (crisis support vs. daily check-ins, intake and triage, between-session support); the “do not attempt” list (diagnosis, medication recommendations, any positioning as clinical authority); conversation flow mapping for your top scenarios (happy path, confused user, angry user, drop-off, re-engagement); technology direction based on risk tolerance, explainability needs, and ops overhead; pilot success metrics (completion rate, handoff rate, safety flag rate, retention).
- Outputs: Scope doc, flow diagrams, risk register, and a first-pass safety policy that defines what triggers escalation, what gets blocked, and what gets handed to a human.
- Cost: $5,000 to $10,000.
Weeks 3-4: Design Conversation Flows and Clinical Content
- Goal: Build the clinical voice, guardrails, and escalation logic before you wire any of it into a platform.
- Cover: Library of 100+ therapeutic responses organized by intent (validation, reframing, grounding, next-step prompts); crisis escalation protocols (when to stop, when to hand off, how to route the user to real-time help); review by clinical psychologists for tone, safety, and appropriateness; clear refusal patterns for diagnosis and medication questions.
- Outputs: Response library, intent taxonomy, escalation decision tree, and a review log (what was approved, what was rejected, why).
- Cost: $8,000 to $15,000.
Weeks 5-6: Build the Core Chatbot Architecture
- Goal: Implement the core conversational system in a way that’s testable and maintainable.
- Cover: NLP/LLM platform setup; conversation state model (what the bot remembers and what it forgets); conversation flow implementation; fallback handling for unclear input, off-topic messages, and repetitive loops; logging and analytics baseline; one channel only for the pilot (multi-channel too early is a tax).
- Outputs: Working chatbot in a staging environment, baseline logging and analytics in place, admin tooling for content updates, and a stub handoff path you’ll wire up properly in the next two weeks.
Weeks 7-8: Add Safety Guardrails and Human Handoff
- Goal: Layer the safety architecture and operational handoff on top of the working chatbot, before any real user sees it.
- Cover: Deterministic risk detection on every turn; a policy gate that runs before the LLM responds; response mode selection (normal, restricted, escalation); a hard-coded crisis resources card; human handoff workflow with after-hours behavior defined; runtime output validators that block diagnosis, medication, and other disallowed content; escalation event logging with triggers and outcomes.
- Outputs: Working safety pipeline integrated end-to-end, documented escalation routing (including 2 AM behavior), audit-ready logs, and clinical sign-off on the implemented safety policy.
Weeks 9-10: Test Edge Cases, Safety, and User Experience
- Goal: Prove the bot behaves safely in edge cases, not just in curated demos.
- Cover: Testing across 50+ scenarios including adversarial inputs, slang, ambiguity, and “user says nothing useful”; clinical review of responses as implemented (things change once the bot is stitched together); edge case handling (retries, escalation loops, refusal behavior, safe exits); user acceptance testing with the intended audience and stakeholder sign-off.
- Outputs: Scenario test suite, issue backlog tagged by severity, approved release criteria, and a “known limitations” statement you’re willing to publish.
Weeks 11-12: Launch a Controlled Pilot
- Goal: Ship a controlled pilot with support readiness and compliance basics in place.
- Cover: HIPAA compliance audit, or a documented rationale if HIPAA doesn’t apply (either way, write it down); terms of service finalization and user-facing disclaimers in plain English; support documentation covering escalation routing, incident response, and on-call ownership; soft launch with beta users, monitored hours, and a documented rollback plan.
- Outputs: Pilot release, monitoring dashboard, support runbook, and a week-by-week iteration plan based on real transcripts and metrics.
Safety and Ethical Considerations for Mental Health Chatbots
If your bot is allowed anywhere near mental health, safety isn’t a “nice to have.” It’s the product. The rest is UI.
You’re building a system that will sometimes meet users on their worst day. That means you need two things at all times: (1) early detection when the conversation is becoming unsafe, and (2) a deterministic way to get a human (or emergency resources) involved—without relying on the bot to “say the right thing.”
Safety Protocols & Crisis Escalation Logic
A safety-first mental health chatbot isn’t “an LLM with a disclaimer.” It’s a layered system where the model is one component, and it loses control the moment risk goes up.
A simple reference architecture looks like this:
Intake, Risk Signals, and Early Detection
– Run lightweight detection on every turn: keyword hits, patterns (intent + phrasing), and simple sentiment/urgency signals.
– Goal: catch indirect distress and “coded” language, not just obvious phrases.
Policy Gates and Deterministic Overrides
– Before any response is generated, route the message through a rules/policy layer.
– If high-risk conditions are met, the bot does not “think harder.” It switches modes.
Response Mode Selection: Normal, Restricted, and Escalation Modes
– Normal mode: the LLM can respond, but only within allowed boundaries.
– Restricted mode: the LLM is constrained to a narrow set of safe responses (grounded, non-clinical, no diagnosis).
– Escalation mode: the LLM is bypassed and you show a hard-coded crisis resources card and a clear next step.
Human-in-the-Loop Handoff
– For practice-owned bots: escalation may route to a live therapist, an on-call workflow, or a warm transfer to your practice’s support channel.
– For public-facing bots: escalation often means a structured handoff (schedule/callback flow) plus emergency resources when appropriate.
– Design principle: no bargaining, no “are you sure?” loops, no delays.
Guardrails Against Unsafe Output
– Add an “anti-hallucination” layer: validators and content filters that block disallowed categories (e.g., diagnosis, medication recommendations, or content that reinforces delusional beliefs).
– This can be implemented via vendor guardrails frameworks (e.g., NVIDIA NeMo Guardrails) or application-level validators (e.g., LangChain-style output checks), but the idea is the same: enforce policy at runtime, not by hope.
Logging, Review Hooks, and Audit Trails
– Keep session transcripts for clinical review only if you can secure them: strong access controls, minimal retention, strict permissions, and audit trails for access.
– Log every escalation event (what triggered it, what happened next) so you can run incident triage and improve the rules.
Critical Safety Features Every Mental Health Chatbot Needs
- Crisis detection that’s more than a keyword list. Start with keywords, yes, but back it with patterns (intent + phrasing) and simple sentiment/urgency signals so you’re not blind to “coded” language or indirect distress.
- Automatic escalation to human support. Define triggers and route users to a real person (or a real-time support workflow) fast. No bargaining, no “are you sure?” loops, no delays.
- Disclaimers that users actually read. Put limitations where decisions happen (first use, and before sensitive flows), in plain language: what it can do, what it can’t, and what to do in emergencies.
- Crisis hotline integration. Make emergency options one tap away in any “unsafe” path, not buried in a footer. If you operate across regions, don’t hardcode a single number. Use location-aware routing or a clear regional selector.
- Session transcripts for clinical review (with strong access controls). Logs are how you improve safety, catch failure modes, and prove oversight. But treat transcripts as sensitive by default: minimal retention, strict permissions, and audit trails for access.
Ethical Guidelines for Mental Health Chatbot Development
- Never diagnose or prescribe. Your bot can reflect, validate, and suggest next steps. It cannot label conditions, recommend meds, or position itself as clinical authority.
- Always identify the bot clearly. No “I’m your therapist” cosplay. Users should understand they’re interacting with software, every time.
- Privacy by design (HIPAA where applicable). If there’s any chance you’re handling PHI, architect for HIPAA-grade controls from day one: least-privilege access, encryption, auditing, and vendor agreements where required.
- Informed consent isn’t a checkbox. Make consent explicit and specific: what data you collect, how it’s used, who can see it, and how to revoke access or delete data.
- Regular clinical oversight. A mental health chatbot without ongoing review is basically “ship and pray.” Set a cadence for clinician review, incident triage, and content updates, especially after edge-case failures.
A useful gut-check: if you can’t explain your escalation rules, your data boundaries, and your review process in one page, you’re not “being thorough.” You’re hiding the sharp edges.
Regulatory Compliance Guide for Mental Health Chatbots
Compliance for mental health chatbots in 2026 is not one rule. It’s a stack: HIPAA when you handle electronic protected health information (ePHI), FDA when you start to make clinical claims, state consumer health data laws regardless of HIPAA, the FTC Health Breach Notification Rule on top, AI transparency laws in select states and the EU, and SOC 2 if you want to sell into anything that looks like an enterprise.
The goal of this section is not to make you a regulatory lawyer. It’s to give you the right mental model for how these layers fit together, so you can scope an MVP without painting yourself into a corner you’ll have to rip out later.
Before you can pick the right rules to follow, you have to figure out what kind of product you’re building. That’s where this starts.
Start With Product Classification: Wellness Tool, Healthcare Tool, or SaMD?
The most common mistake teams make is choosing a regulatory path before they’ve classified the product. Three buckets matter.
Wellness tool. General mental wellness positioning, no clinical claims, no diagnosis, no treatment. Sold direct to consumer or B2B (employer wellness, university EAP). Lighter regulatory load: state consumer health data laws, FTC, AI transparency requirements, plus baseline security hygiene. HIPAA usually does not apply unless a covered entity is involved.
Healthcare tool. Used inside a HIPAA-regulated workflow (a clinic, a payer, a covered entity), even if the product itself doesn’t make clinical claims. As soon as ePHI flows through your system, HIPAA applies, you need a Business Associate Agreement (BAA) with the covered entity, and your security and privacy controls have to meet the bar.
Software as a Medical Device (SaMD). The product makes clinical claims (diagnosis, treatment, clinical decision support), or otherwise meets the FDA’s definition of a medical device. This is the heaviest path. The IMDRF defines SaMD as software intended for medical purposes that performs without being part of a hardware device, and the FDA applies risk-based oversight on top of it. SaMD products require Quality Management System (QMS) practices and, depending on classification, FDA submission and clearance.
Three quick lenses to triangulate which bucket you’re in:
Who You Sell To
If you’re selling B2B to clinics, payers, or hospital systems, you’re almost certainly in the healthcare bucket and HIPAA-on by default. If you’re selling B2C or to employers as a wellness perk, you’re in wellness territory unless your claims push you into SaMD.
What Data You Touch
If you’re handling ePHI (protected health information in electronic form, tied to an identifiable person, in a HIPAA-regulated workflow), HIPAA applies. If you’re handling sensitive mental health data outside a HIPAA-regulated workflow, you’re not exempt; you’re under the FTC and state consumer health data regimes. The “we’re not HIPAA so we’re fine” argument is almost always wrong.
What Claims You Make
The fastest way to escalate yourself from wellness to SaMD is to make clinical claims. “Helps with stress” is wellness language. “Treats moderate depression” is medical device language. Marketing copy is regulatory copy. Your website is part of the regulatory perimeter.
HIPAA Requirements When You Handle ePHI
If you’re touching ePHI, HIPAA is the floor, not the ceiling. The Security Rule defines administrative, physical, and technical safeguards; the Privacy Rule governs use and disclosure; the Breach Notification Rule kicks in when something goes wrong. Below is the operational version of what that means for a chatbot.
Technical Safeguards
- Encryption in transit (TLS 1.2+) and at rest (AES-256 or equivalent).
- Access controls with least-privilege defaults, MFA for any human accessing PHI.
- Audit logging of every read, write, and export of ePHI, retained per your policy.
- Secure session handling with automatic timeouts and re-authentication.
- Backup, recovery, and disaster recovery procedures that are tested, not just documented.
Process And Governance Requirements
- Business Associate Agreements (BAAs) with every vendor that touches ePHI on your behalf, including LLM providers when applicable.
- A formal risk analysis and risk management program, refreshed at least annually and after material changes.
- Workforce training, sanctions for violations, and a documented incident response plan.
- A breach notification process that meets the 60-day requirement and the documentation standard behind it.
Practical Data Handling Rules
- Minimum necessary use: the bot, the LLM, and your team should only see the data they actually need.
- De-identify anywhere you can. Aggregate analytics, model improvement, and most internal tooling can run on de-identified data.
- Be explicit about what crosses provider boundaries. Sending PHI to a third-party LLM API without a BAA is a HIPAA violation, period.
- Have a clear retention and deletion policy, and enforce it in code, not just in a policy document.
Also Read: How to Develop a Natural Language Processing App
FDA Considerations For AI Mental Health Chatbots
Whether the FDA cares about your chatbot depends almost entirely on your intended use: what you say it does, what you market it as, and the conditions under which it’s used.
Low-Risk Guardrails If You Want To Stay In Wellness Territory
If your goal is to ship a general mental wellness product without an FDA pathway, design and document accordingly:
- Clear, consistent wellness positioning across product, marketing, and onboarding. No therapeutic claims, no diagnosis language, no treatment language.
- No personalized treatment recommendations. The bot can offer general psychoeducation and skills, not “your treatment plan.”
- Disclaimers that the product is not intended to diagnose, treat, cure, or prevent any disease, surfaced where users would form expectations, not buried in legal pages.
- Audit trail showing how you arrived at “wellness” classification, including marketing review.
What Changes If The Product May Be Regulated As SaMD
If your product makes clinical claims, supports clinical decision-making, or is used to diagnose or treat, it’s likely SaMD, and the bar is much higher.
- Risk classification based on the IMDRF framework (significance of the information and seriousness of the condition).
- Quality Management System (QMS) aligned with FDA expectations (commonly ISO 13485-style practices).
- Software lifecycle controls: design history, verification and validation, traceability, change management.
- Premarket submission pathway: 510(k), De Novo, or PMA depending on classification, with the FDA’s Pre-Cert and Software Pre-Submission programs as relevant on-ramps.
- Real-world performance monitoring and post-market surveillance.
Practical reality: if you’re not certain whether you’re SaMD, get a regulatory consult before you ship. The cost of a wrong call goes up sharply once the product is in users’ hands.
State Privacy Laws And Not-HIPAA Traps
One of the most expensive misreads in this space is “we’re not HIPAA, so we’re fine.” You’re not. Several state laws and one federal rule apply to consumer mental health data outside HIPAA, and they apply specifically to the kind of data a wellness chatbot collects.
Consumer Health Data Laws
Washington’s My Health My Data Act and similar state-level laws define “consumer health data” broadly enough to cover mental health symptoms, mood data, and inferences drawn from chatbot conversations. Requirements typically include:
- Explicit, opt-in consent before collection.
- A separate, prominent consumer health data privacy policy (not buried in a general privacy policy).
- Strict limits on selling or sharing consumer health data with third parties.
- Granular user rights: access, correction, deletion, withdrawal of consent.
- A private right of action in some states, which means individual users can sue.
California, Connecticut, Nevada, Texas, and others have their own variations, and the trend is toward more states, not fewer. If you’re national, plan for the strictest applicable rule.
FTC Health Breach Notification Rule
The FTC’s expanded Health Breach Notification Rule applies to vendors of personal health records and related entities, including most consumer mental health apps that don’t fall under HIPAA. Practically, that means:
- Notification obligations within 60 days of a breach (to affected users, the FTC, and in some cases the media).
- Coverage of “unauthorized disclosure,” not just hacks. Sharing data with a third-party advertising or analytics SDK without proper authorization can itself be a notifiable breach.
- Real enforcement risk. The FTC has taken multimillion-dollar actions against mental health companies for tracking pixels and analytics SDKs that leaked health data to ad platforms.
The simple defense: audit every third-party SDK, pixel, and integration for what it sees, get explicit consent where required, and assume the FTC means it.
Telehealth, Minors, and Special Data Categories
A few extra layers are worth flagging:
- Telehealth-specific state regulations may apply when your product is positioned as part of a clinical workflow.
- COPPA applies if any portion of your product is directed at users under 13 (and several states have layered teen-specific protections on top).
- Substance use disorder records are protected under 42 CFR Part 2, which has stricter consent and disclosure rules than HIPAA.
- Suicide-related data, abuse disclosures, and similar categories often carry mandatory reporting obligations depending on jurisdiction and the role of the user (clinician vs. consumer).
AI Transparency and Bot Disclosure Requirements
A separate stack of rules has emerged in 2025 and 2026 specifically about AI: who has to know they’re talking to one, what the system has to disclose, and what the system is allowed to claim about itself.
EU AI Act: If You Plan European Markets
The EU AI Act applies risk-based requirements to AI systems on the EU market. For a mental health chatbot:
- Most products will fall in the “limited risk” tier, which mandates clear disclosure that the user is interacting with AI.
- Systems that perform something close to clinical decision support, or that are integrated into healthcare workflows, may be classified as “high risk,” with documentation, conformity assessment, post-market monitoring, and human oversight obligations.
- “Manipulative” AI practices and certain forms of emotion recognition are restricted or prohibited outright depending on context.
If European users are anywhere in your roadmap, design for the AI Act now. Retrofitting it later is more painful than getting it right from the start.
Bot Disclosure Laws and Companion AI Rules
Several US states have or are passing laws that require bot disclosure or impose specific obligations on companion AI:
- California’s SB 1001 requires disclosure for bots used to incentivize purchases or influence votes; broader bot-disclosure proposals continue to advance.
- California SB 243 imposes specific obligations on operators of “companion AI” used by minors and includes safety, disclosure, and reporting requirements.
- Other states are following, often with overlapping but non-identical definitions.
The defensible posture: always identify the bot as AI, in plain language, on first interaction and any time the user might reasonably forget. Don’t roleplay as human even when users beg you to. The lawsuits and regulatory actions in this space are mostly about products that blurred that line.
SOC 2 and Enterprise Trust Requirements
If you plan to sell to employers, payers, health systems, universities, or any decent-sized B2B buyer, you’ll be asked for a SOC 2 report. It’s not legally required the way HIPAA is, but you cannot win enterprise deals without one.
Why SOC 2 Matters for Employer and Enterprise Deals
SOC 2 is a third-party attestation that you actually do what you say you do for security and (optionally) availability, processing integrity, confidentiality, and privacy. For mental health chatbot development specifically, it matters because:
- Procurement teams use SOC 2 as a baseline filter. No report, no deal.
- Health systems and payers will pair SOC 2 with HIPAA evidence, not substitute one for the other.
- Employer wellness buyers care about privacy and confidentiality criteria specifically, given how sensitive the data is.
Plan for SOC 2 as a 6 to 12 month effort, not a sprint. Doing it before you have customers is hard; doing it without a security program is impossible.
SOC 2 Type I Vs SOC 2 Type II
- SOC 2 Type I: a point-in-time assessment of whether your controls are designed appropriately. Faster and cheaper, useful as an initial signal.
- SOC 2 Type II: an assessment of whether your controls operated effectively over a period (typically 6 to 12 months). This is what serious enterprise buyers want.
The pragmatic order is usually Type I first to unblock early enterprise deals, then Type II as soon as you have a clean operating window.
What Good Compliance Looks Like in Practice
Layering all of the above is intimidating on paper, but in production it tends to look the same across the products that get this right. A useful gut-check:
- Product classification is documented, signed off internally, and consistent with marketing.
- HIPAA, where it applies, is enforced in code (encryption, access control, retention) and in process (BAAs, risk analysis, training, incident response).
- Wellness products treat consumer health data laws and the FTC Health Breach Notification Rule as the actual floor, not an afterthought.
- AI is disclosed clearly and consistently, and the product never roleplays as a human or as a clinician.
- Crisis resources are deterministic, not LLM-generated, and surface immediately when escalation triggers.
- SOC 2 (or an equivalent attestation) is in flight or in hand if there’s any enterprise plan.
- The whole compliance posture is reviewed at least annually and after every material product change.
If a regulator, an enterprise buyer, and a clinical reviewer would each independently nod at your compliance posture, you’re in the right place. If any one of them would walk out of the room, the gap is the work.
Mental Health Chatbot Architecture and Tech Stack
A modern mental health chatbot is not a single component. It’s a layered system, and the layers each do a specific job. The diagram earlier in this guide shows how the pieces fit together; this section walks through each layer and the technical decisions inside it.
The right way to think about the stack: every user message flows through the same path, every time, and the safety layers are in the path, not bolted on after.
Core Architecture: from User Message to Safe Response
The path a single message takes in a production-grade mental health chatbot looks like this:
- User input lands in the system (text, voice transcribed via STT, or webhook requests from an integrated channel).
- NLU and risk detection run together to extract intent, entities, sentiment, and risk signals.
- The policy and safety gate runs before the LLM, applying deterministic rules: is this a crisis? Is this a disallowed topic (diagnosis, medication)? Should we restrict, escalate, or proceed?
- If the gate clears, the request goes to the LLM with retrieval-augmented generation (RAG) and relevant memory context.
- The LLM’s draft response runs through output validators that block unsafe or out-of-scope content.
- The validated response goes back to the user. If the gate triggered escalation in step 3, the LLM is bypassed entirely and a deterministic crisis or handoff flow runs instead.
The point is that the LLM is one component in a larger pipeline, not the brain of the operation. The deterministic layers around it are what make the system shippable in healthcare.
LLM Layer: Response Generation and Reasoning
The LLM is responsible for the actual response generation: producing fluent, contextually appropriate, on-brand replies. In 2026, the realistic options break down into three buckets.
Frontier hosted models. GPT-4 / GPT-4o, Claude, Gemini. Strongest reasoning and tone, fastest to ship, lowest control. For HIPAA workflows you need a BAA from the provider. Pricing is per-token and adds up at scale, especially with long context windows.
Open-weight models you host yourself. Llama 3, Mistral, and similar. Lower per-message cost, much more control, but you own the infrastructure, the latency curve, and the safety tuning. This route only makes sense if you have ML engineering capacity and a real reason to need it (data residency, custom fine-tuning, or volumes that make hosted economics painful).
Specialized or fine-tuned models. A frontier or open-weight base, fine-tuned on a tailored dataset of approved clinical content and tone examples. Useful for locking in voice and reducing prompt-engineering load, but fine-tuning is a maintenance commitment, not a one-time event.
The pragmatic default for most teams in 2026: start with a hosted frontier model behind a strong system prompt, retrieval, and runtime guardrails. Move to self-hosting or fine-tuning only when you have data showing it’s worth the operational cost.
RAG Layer: Grounding Responses in Approved Clinical Content
RAG is what keeps the LLM saying things you’d actually want it to say. Instead of relying purely on whatever the model learned during pretraining, you ground each response in your own approved knowledge base.
A practical RAG layer for a mental health chatbot looks like this:
- A curated content library of clinically reviewed material: psychoeducation, CBT exercises, grounding scripts, mindfulness prompts, escalation copy, FAQ.
- An embeddings pipeline that converts each piece of content into a vector and stores it in a vector database (Pinecone, Weaviate, pgvector, Qdrant, etc.).
- Retrieval logic that, on every turn, pulls the most relevant chunks for the current user state and intent.
- A prompt template that instructs the LLM to base its response on the retrieved content and to refuse if the retrieved content doesn’t cover the question.
Done well, RAG is your strongest anti-hallucination mechanism. The model is no longer riffing from training data; it’s drafting from material your clinical reviewers signed off on.
Two non-obvious points:
- Retrieval is a product problem, not just an infra problem. The quality of your chunks, the metadata you tag them with, and the queries you build to retrieve them matter more than the specific vector DB.
- Frameworks like LangChain and LlamaIndex are useful for moving fast, but the abstraction can hide the things you actually want to inspect (which chunks were retrieved, why, with what scores). Build for visibility into retrieval from day one.
Memory Layer: What the Bot Should Remember and Forget
Memory is where many mental health chatbots quietly create problems. Without thinking carefully, teams either remember too little (the bot feels like a stranger every session) or too much (you’re now sitting on a large pile of sensitive data with unclear retention rules).
A defensible memory model has three layers:
- Session memory. What the user said in this conversation. Short-lived, tied to the active session, used for context within the dialog.
- User profile memory. Stable preferences and high-level context (preferred name, time zone, what’s worked for them in the past). Should be explicit, user-visible, and editable.
- Clinical context. Things that matter clinically (recent mood scores, completed exercises, escalation history). Should be on a separate retention policy from chat history, with stricter access controls.
Rules of thumb:
- Default to less memory, not more. Memory you don’t have can’t leak.
- Make memory user-visible and user-controllable. “What does the bot remember about me?” should have an actual answer.
- Treat clinical content like clinical content. Don’t store mood scores or symptom data in the same bucket as light product preferences.
Safety and Monitoring Layer
The safety layer is the architectural ground truth that makes a mental health chatbot a healthcare product instead of an experiment.
What lives here:
- Pre-LLM policy gate. Deterministic checks (intent classification, risk scoring, disallowed topic detection) that run on every user message before the LLM is invoked.
- Runtime guardrails. Frameworks like NeMo Guardrails, Guardrails AI, or in-house validators that constrain LLM behavior at runtime: blocking diagnosis language, preventing medication advice, enforcing escalation flows.
- Output validators. Post-generation checks that catch unsafe content before it reaches the user.
- Crisis routing. Hard-coded crisis flows that bypass the LLM entirely when escalation triggers, surfacing approved crisis resources without model debate.
- Logging and audit trail. Every escalation event, every blocked output, every handoff, with enough detail for clinical review.
- Continuous monitoring. Dashboards for safety incidents, drift in model behavior, and unusual conversation patterns.
The principle to internalize: the LLM is the part you can’t fully control, so the rest of the architecture has to be designed around that fact.
Read more on conversational AI in healthcare.
Integration Layer: Apps, EHR, Scheduling, and Support Tools
The last layer is how your chatbot connects to the rest of the world. For a wellness app, this layer is light. For a clinical product, it’s a meaningful chunk of the engineering work.
Common integrations:
- Front-end channels. Mobile and web apps, voice assistants, messaging platforms (WhatsApp, SMS, Messenger), embedded widgets in patient portals.
- EHR and clinical systems. FHIR-based integration into the clinician’s workflow so chatbot summaries, risk events, and engagement data show up where the clinician already lives.
- Scheduling and triage. Calendar systems, on-call rotations, EAP partner APIs, warm-transfer flows.
- Support tooling. Ticketing, case management, and human handoff routing for non-crisis but high-touch situations.
- Analytics and BI. De-identified pipelines for aggregate reporting to product owners, B2B buyers, and clinical leadership.
The integration layer is also where compliance shows up most operationally: every external system that touches PHI needs a BAA and a documented data flow, and every third-party SDK in the front-end client is in scope for the FTC Health Breach Notification Rule.
Looking to design a stack like this without rebuilding from scratch? We help product teams ship mental health chatbots end to end.
Best Tools And Platforms For Mental Health Chatbot Development
Mental health chatbot development in 2026 doesn’t come down to one platform versus another. The right choice depends on how much control you need, where the conversation logic lives (deterministic flows vs. open-ended LLM reasoning), and what kind of compliance posture you’re committed to. Below are the six tool categories that actually matter for building and operating a mental health chatbot today, with the trade-offs that decide which fits your build.
Dialogflow ES For Simple Goal-Oriented Flows
Dialogflow ES (Essentials) is Google’s original, lighter-weight conversational AI platform. It’s well suited to chatbots where the conversation is mostly goal-oriented: structured intake forms, scheduling, FAQ flows, simple mood check-ins.
Where it fits:
- You need fast prototyping and a clean intent/entity model out of the box.
- Your conversation logic is mostly linear or has a small number of well-defined branches.
- You don’t need complex state management, multi-step reasoning, or sophisticated memory.
Where it falls short for mental health: Dialogflow ES doesn’t give you the safety architecture a serious mental health chatbot needs (deterministic policy gates, output validators, escalation routing). You can build those layers around it, but at that point you’re maintaining most of the safety stack yourself anyway.
Related: Medical Chatbots: Use Cases in the Healthcare Industry
Dialogflow CX For Complex Branching Conversations
Dialogflow CX is the heavier sibling. It uses a state-machine model that handles complex branching, long flows with shared sub-flows, and richer context management. For mental health products that need structured, multi-step conversations (CBT exercises, multi-day check-in series, intake-to-triage flows), CX is a substantially better fit than ES.
Strengths:
- State machine model maps cleanly to clinical flows that have explicit stages and conditions.
- Visual flow builder makes clinician-engineer collaboration realistic, not just a slide-deck idea.
- Strong integration story with Google Cloud, including the security and compliance tooling enterprise buyers expect.
Caveats:
- Learning curve is steeper than ES; budget time for the team to actually become fluent.
- You’re still bringing your own LLM layer, RAG, runtime guardrails, and crisis flows on top of CX. CX is the dialog backbone, not the whole stack.
Related: How To Build Your Own ChatGPT Chatbot
Rasa for High-Control and Self-Hosted Chatbots
Rasa is the open-source conversational AI framework of choice for teams that need maximum control and on-premise or private-cloud hosting. For HIPAA-regulated workflows, regulated markets, or any product where data residency is a constraint, Rasa is often the only realistic platform option.
Why teams pick Rasa:
- Self-hosted by default. Your data, your infrastructure, your audit trail.
- Mature NLU with strong support for intents, entities, and custom pipelines.
- A flexible dialog management model (Rasa NLU + Rasa Core) that can be extended to fit clinical workflows.
- Active ecosystem of integrations and a real community around it.
The trade-off is that Rasa demands more engineering. You’re trading hosted convenience for control, which is the right deal for some products and the wrong one for others. Pair Rasa with an LLM layer (hosted or self-hosted) when you want generative responses on top of structured dialog management.
Related: How is ChatGPT Used in Healthcare
LLM APIs for Flexible AI-Powered Support
For most teams shipping a mental health chatbot in 2026, the practical starting point is a hosted LLM API: OpenAI (GPT-4, GPT-4o), Anthropic (Claude), Google (Gemini). The model handles natural language understanding and generation in one call, and you build the rest of the stack around it.
What this approach buys you:
- Strongest reasoning and tone available, with no infrastructure burden.
- Fast iteration on prompts, retrieval, and guardrails without retraining cycles.
- Clear path to compliance: providers offer BAAs and HIPAA-eligible endpoints (verify the specific tier you’re on).
What you have to build around it:
- Pre-LLM policy gates and risk detection.
- RAG over your approved clinical content (the LLM should not be making things up about CBT or grounding exercises).
- Runtime guardrails and output validators that constrain what the model is allowed to say.
- Logging and audit trail at the model-call layer.
The honest framing: an LLM API gets you 70% of a chatbot. The remaining 30% (safety, retrieval, integrations, ops) is where the engineering actually happens.
Private or Self-Hosted LLMs for Enterprise Control
For enterprise buyers, certain regulated markets, or products with extreme data residency requirements, hosted LLM APIs aren’t always an option. Self-hosted open-weight models (Llama 3, Mistral, and similar) let you run inference inside your own VPC or on-prem.
When this is the right call:
- Health systems or payers that won’t approve a third-party LLM provider, even with a BAA.
- Markets with hard data residency rules (EU, certain regions in APAC, regulated government contexts).
- High-volume products where hosted economics get painful and self-hosted starts to pencil out.
- Products that need deep fine-tuning on a tailored dataset and want full ownership of the resulting weights.
The cost is real: GPU infrastructure, latency tuning, model evaluation pipelines, and ongoing safety tuning. This route only makes sense if you have ML engineering capacity and a real reason to need it. For most early-stage products, a hosted frontier model with strong guardrails wins.
Guardrails Frameworks And Runtime Validators
Whatever model you use, you don’t ship a mental health chatbot without a runtime guardrails layer. This is the layer that keeps the LLM from drifting into diagnosis, medication advice, or unsafe responses.
Options worth knowing:
- NeMo Guardrails (NVIDIA). Programmable guardrails framework with a DSL for defining conversational rails, fact-checking, and topic restriction.
- Guardrails AI. Python-first framework for validating LLM outputs against structured schemas and policies, with a growing library of validators.
- In-house validators. Many production mental health chatbots run a thin custom layer on top of (or instead of) the off-the-shelf frameworks, because the rules are product-specific and the audit trail needs to be tight.
What a usable guardrails layer should give you:
- Pre-call topic and risk classification.
- Post-call output validation (no diagnosis language, no medication recommendations, no unsafe content).
- Deterministic escalation routing when crisis triggers fire.
- Clear logs of every block, every override, every escalation, ready for clinical and compliance review.
If your guardrails layer can’t answer “what did the bot refuse to say, and why” for a given conversation, it isn’t ready for production.
Which Mental Health Chatbot Platform Should You Choose?
Choosing a platform for mental health chatbot development comes down to three questions, in order: what kind of conversation are you building, what are your safety and data constraints, and which platforms actually fit those answers? Work through them in that order and the shortlist usually picks itself.
Start With the Conversation Type
Before you compare platforms, get specific about the conversation. The right platform for a structured intake-and-triage flow is rarely the right platform for an open-ended journaling companion.
A few lenses that help:
- Goal-oriented vs. open-ended. Are users coming in with a specific task (book an appointment, complete a check-in, run a CBT exercise), or with a vague need they want to talk through? Goal-oriented flows do well on platforms with strong dialog management (Dialogflow CX, Rasa). Open-ended conversations lean on LLM APIs with retrieval and guardrails.
- How much state matters. A one-off mood check-in needs almost no state. A 21-day program with branching content needs serious state management.
- How much variation in response is acceptable. Crisis flows, disclaimers, and routing should be deterministic and templated. General psychoeducation can tolerate (and often benefits from) LLM-generated variation, as long as it’s grounded in approved content.
Get this right and the platform shortlist narrows fast. Most teams that struggle here are trying to use one platform for two very different conversation types in the same product.
Check Safety, Data, and Hosting Requirements
The next filter is non-negotiable: where does your data live, who can see it, and what does your compliance posture demand?
Run your shortlist through these checks:
- HIPAA and BAA availability. If you’re handling ePHI, the platform (and any LLM provider behind it) must offer a BAA on a tier you can actually afford.
- Hosting and data residency. Self-hosted only? VPC deployment required? EU data residency? These constraints knock out most hosted-only platforms immediately.
- Audit and logging support. Can you produce a complete record of every conversation, every escalation, and every model output for clinical and regulatory review?
- Guardrails compatibility. Does the platform play well with the runtime guardrails layer you plan to use, or does it lock you into its own opinionated stack?
- Integration footprint. EHR (FHIR), scheduling, EAP partner APIs, ticketing, analytics: the more clinical your product, the more these matter.
If a platform fails any of these checks for your use case, it doesn’t matter how good the rest of it is. Move on.
Compare the Main Platform Options
With conversation type and safety constraints in hand, the comparison becomes practical. Here’s the simplified version of how the main options stack up for mental health chatbot development:
| Platform | Best For | Customization | Hosting | Watch-Outs |
|---|---|---|---|---|
| Dialogflow ES | Simple goal-oriented flows, fast prototypes | Low to moderate | Hosted (Google Cloud) | Limited safety architecture; you’ll build most guardrails yourself |
| Dialogflow CX | Complex branching clinical flows | Moderate to high | Hosted (Google Cloud) | Steeper learning curve; still need LLM + guardrails on top |
| Rasa | High-control, self-hosted, regulated workflows | Very high | Self-hosted or private cloud | Highest engineering investment; pair with an LLM layer for generative responses |
| Hosted LLM APIs (OpenAI, Anthropic, Google) | Open-ended conversations, fast iteration, strong reasoning | High (via prompts, RAG, guardrails) | Provider-hosted (BAA-eligible tiers) | You build the safety stack around the model |
| Self-hosted open-weight LLMs (Llama 3, Mistral) | Strict data residency, enterprise control, fine-tuned models | Very high | Self-hosted (your VPC or on-prem) | Significant infrastructure and ML engineering commitment |
| Guardrails frameworks (NeMo, Guardrails AI) | Runtime safety layer on top of any model | High | Lib-level, deploys with your stack | Not a chatbot platform on their own; pair with one of the above |
The pattern that works for most teams in 2026: pick a primary dialog or model platform that fits your conversation type and hosting constraints, then layer a guardrails framework and a thin custom safety layer on top. Don’t pick on raw capability alone. Pick on what you can actually operate, audit, and defend in front of a clinician and a compliance reviewer.
Mental Health Chatbot Examples: What Product Teams Can Learn From Them
Looking at what’s already in market is the fastest way to calibrate your own product. The four examples below cover most of the design space for mental health chatbots in 2026: a digital therapeutic on an FDA path, a hybrid AI-plus-human support model, an enterprise-grade text-based companion, and a consumer companion that ran into the limits of weak guardrails. Each one teaches a different lesson worth stealing.
Woebot: Structured CBT Support With A Digital Therapeutic Path

- Product model: Mobile app delivering structured cognitive behavioral therapy (CBT) interactions, originally direct-to-consumer, increasingly positioned as a digital therapeutic for clinical and enterprise channels.
- What it does: Daily check-ins, mood tracking, CBT-style exercises (thought reframing, behavioral activation), and psychoeducation, all delivered through a tightly scripted conversational experience rather than open-ended LLM chat.
- Evidence / regulatory signal: A randomized controlled trial published in JMIR Mental Health found that college students using Woebot had significant reductions in depression symptoms (PHQ-9, d=0.44) over two weeks vs. an information-only control. Woebot Health also received FDA Breakthrough Device designation for WB001 (postpartum depression), which signals serious intent on the digital therapeutic path.
- Business model: Mix of B2C subscription and B2B partnerships with health systems, payers, and employers, with an FDA-cleared product as the long-term anchor.
- Key product lesson: Tight scripting and clinical rigor beat open-ended chat for outcomes. Woebot’s evidence base exists precisely because the conversation is constrained, not despite it.
Wysa: AI-Led Support For The “Missing Middle”

- Product model: AI chatbot offering CBT-based exercises, mood tracking, and structured emotional support, paired with optional access to human coaches for users who need more.
- What it does: Daily check-ins, guided exercises across anxiety, sleep, and stress, journaling prompts, and an upgrade path to live coaches inside the app. Targeted at the “missing middle”: people who don’t need clinical care but aren’t fine on their own either.
- Evidence / regulatory signal: Wysa has reported 6+ million users globally and published research in JMIR (n=2,061) showing meaningful symptom improvement in depression and anxiety among engaged users. Wysa received FDA Breakthrough Device designation in 2022 for chronic musculoskeletal pain (with comorbid depression and anxiety), one of the more interesting cross-domain expansions in the space.
- Business model: B2B sales to employers and health plans (white-labeled or co-branded), plus consumer subscription. Enterprise revenue has clearly become the priority.
- Key product lesson: A clean upgrade path from AI to human is a real product feature, not just a marketing idea. Wysa wins because it doesn’t pretend the AI alone is enough for everyone.
Tess / X2AI: Psychological Support Through Text-Based Conversations
- Product model: Enterprise-focused, text-based mental health support delivered over SMS and messaging platforms, designed to integrate into existing healthcare and educational workflows rather than as a standalone consumer app.
- What it does: Conversational psychoeducation, emotional support, and structured check-ins, deployed across health systems, universities, and humanitarian programs. Tess has been used by 15+ US universities and in deployments like a 472-message-per-conversation engagement program in Argentina, showing the model holds up across cultures and channels.
- Evidence / regulatory signal: Multiple peer-reviewed studies of Tess deployments in university and clinical settings, generally showing improved engagement and self-reported wellbeing. Less visible in the FDA pipeline than Woebot or Wysa, more visible in academic and humanitarian work.
- Business model: B2B contracts with universities, health systems, NGOs, and enterprise wellness programs. SMS-first design lowers the barrier to deployment in places where app-store-driven distribution doesn’t fit.
- Key product lesson: The right channel often isn’t an app. Meeting users in the messaging tools they already use, with a product designed around that constraint, can outperform a more polished standalone app.
Replika: Companion AI And The Risk Of Emotional Dependency

- Product model: AI companion app offering open-ended conversation, persistent memory, and a customizable AI persona. Positioned for emotional connection and companionship rather than clinical support, but used by many users as de facto mental health support.
- What it does: Long-running, open-ended chat with an AI that “remembers” the user, personalized over time. Optional romantic or “deeper” interaction tiers, voice modes, and AR features.
- Evidence / regulatory signal: Replika has reported 10M+ downloads. In 2023 the Italian Data Protection Authority issued a temporary ban over child safety and data protection concerns and later imposed a €5M fine. Italy moved against Replika again in 2025. The product has become a recurring case study in regulatory and AI-safety conversations about companion AI.
- Business model: Freemium consumer subscription, with paid tiers unlocking deeper interaction features.
- Key product lesson: Companion AI without strong guardrails creates real product and regulatory risk. The combination of open-ended chat, persistent memory, and emotional intimacy is exactly the surface area where mental health failures, regulatory action, and litigation are most likely. If you’re building anywhere in this space, the lesson is to draw the line clearly: emotional support, not emotional dependency, and never roleplay as a clinician or as a human.
Also Read: How to build a chatbot
What Does a Mental Health Chatbot Cost to Build?
If you’ve never shipped clinical-ish software before, the fastest way to blow up your budget is to treat “chatbot” as a single feature. It’s not. The bot is the front door. The expensive part is everything you don’t see: safe data handling, clear conversation boundaries, escalation paths, auditability, and the boring-but-decisive work of making sure the system behaves the same way at 2 PM and at 2 AM.
A more useful way to think about cost is to decide what “done” means for your first release. Is this a self-contained assistant with scripted flows and minimal data retention? A rules engine that needs maintainable conversation logic and analytics? Or an AI-led experience that needs stronger guardrails, monitoring, and a human-in-the-loop fallback? Each step up isn’t just “more smart.” It’s more risk to manage, more QA to run, and more operational load after launch.
The table below isn’t a quote. It’s a scope-to-effort map you can use to sanity-check vendors, align stakeholders, and avoid the classic trap of budgeting for a demo and then discovering you actually needed a product.
| Feature Level | Technology Stack | Development Time | Cost Range | Maintenance/Month |
|---|---|---|---|---|
| Basic Scripted Bot | Dialogflow ES | 2-3 months | $15,000-$30,000 | $500-$1,000 |
| Advanced Rule-Based | Dialogflow CX / Rasa | 4-6 months | $40,000-$80,000 | $1,500-$3,000 |
| AI-Powered (LLM + RAG) | LLM API + Custom guardrails | 6-9 months | $80,000-$150,000 | $3,000-$5,000 |
| Enterprise Clinical | Custom NLP + FDA pathway | 12-18 months | $200,000-$500,000 | $5,000-$15,000 |
A few things worth flagging about how these ranges actually behave in 2026:
- The AI-powered tier is where most teams land for a real mental health chatbot today. The cost is driven less by the model and more by the safety stack (policy gates, runtime guardrails, output validators, audit logging).
- Compliance is a multiplier, not a line item. HIPAA-ready infrastructure, BAAs with vendors, and SOC 2 readiness can add 20-40% on top of the base build, depending on starting point.
- Maintenance is not optional. Ongoing clinical content review, model evaluation, safety incident handling, and compliance refreshes are recurring costs. Underfunding this line is the most common way mental health chatbot products quietly degrade after launch.
Mental Health Chatbot Monetization Models in 2026
Building a mental health chatbot is one problem. Getting paid for it is a separate one. The monetization model you pick shapes your product requirements (especially around safety, clinical oversight, and compliance), your sales motion, and how fast you can actually grow. There’s no universal “best” model in 2026; there are a handful of paths that work, and the right one depends on who you sell to and how clinical your product is.
How to Choose the Right Monetization Model
Before pattern-matching to a model, work through three questions in order:
- Who’s the buyer? A consumer paying $15/month, an employer paying PMPM for 10,000 employees, a clinic paying per-seat, and a payer reimbursing for a digital therapeutic are four entirely different products dressed up to look similar. The buyer dictates the feature set as much as the user does.
- How clinical is the product? “Wellness chatbot” and “FDA-cleared digital therapeutic” sit at opposite ends of the regulatory and evidence stack. The closer you are to the clinical end, the longer the path to revenue and the higher the moat once you get there.
- What’s the procurement reality? Employer wellness, clinic SaaS, and reimbursement each have different sales cycles, different evidence bars, and different operational demands. Pick the one your team is actually positioned to win.
The four models below are the ones that consistently work in 2026. Most products eventually run two of them in combination; very few succeed running all four.
B2B Employee Wellness: Selling Licenses to Corporations
Employer-sponsored distribution is one of the most reliable go-to-market paths in 2026 because demand is unmistakable: in Business Group on Health’s 2024 large-employer survey, 77% of large employers reported increased mental health concerns, and employers were highly focused on access to mental health services.
KFF’s 2024 Employer Health Benefits Survey also shows employers actively expanding access: 48% of large employers increased mental health counseling resources for employees via an employee assistance program (EAP) or third-party vendors, exactly the procurement channel most B2B mental health products plug into.
Employer-sponsored mental wellness platforms are also now common enough to be evaluated in medical literature, which is a good signal you’re not betting your business on a fad.
How teams typically package it:
- Per-member-per-month (PMPM) licensing or annual seat-based contracts.
- Tiered access: “AI support + resources” for the broad population, plus higher tiers for therapy access, care navigation, or higher-touch programs.
- Enterprise buying expectations: security posture (SOC 2 Type II), reporting, and predictable outcomes language (not “our bot is empathetic”).
The trap to avoid: treating the employer as the customer and forgetting that the employee is the user. If the employee doesn’t trust the privacy posture, engagement collapses and the renewal conversation gets ugly.
Freemium Plus Human Support: Free AI Chat, Paid Care Access
This model fits therapist-led offerings because it mirrors how people actually test care: they want a low-friction first step before committing.
A common structure:
- Free: AI chat for intake, psychoeducation, check-ins, lightweight skill practice, and routing.
- Paid subscription: human therapist video sessions (or messaging) bundled with AI support between sessions.
Why it works:
- The AI layer lowers the barrier to starting care (stigma plus scheduling friction), while the paid tier anchors value in what clients ultimately trust most: a licensed clinician.
- It aligns with “hybrid care” operations: AI does the repetitive front door; clinicians focus on the moments that need judgment.
- Conversion economics are favorable when the AI experience genuinely helps. Users who feel real benefit in the free tier convert to paid care at meaningfully higher rates than cold-traffic-to-therapist funnels.
What kills this model: a free AI tier that’s too limited to be useful, or so generous it never produces a reason to upgrade. The pricing line has to sit where the AI experience is genuinely helpful but a human is clearly the next step for users who need more.
Provider or Practice SaaS: Selling Workflow Tools to Clinics
A growing model in 2026 is selling the chatbot (and its admin layer) directly to clinical practices, group therapy clinics, and behavioral health platforms as a workflow tool. The buyer is the practice owner or clinical operations lead; the users are the clinicians and their clients.
What the product looks like in this model:
- Intake and triage flows the practice can configure for their populations.
- Between-session support for the clinician’s existing clients.
- Admin dashboards for clinical review, content updates, and safety incident handling.
- Integrations with the EHR, scheduling, and billing systems the practice already uses.
Pricing typically lands in one of two shapes:
- Per-clinician seat licensing. Predictable for the practice, simple to expand.
- Per-active-client pricing. Aligns cost with usage, useful for practices with variable caseloads.
This model has lower per-deal revenue than enterprise B2B, but the sales cycle is shorter and the product feedback loop is much tighter. Practices will tell you within a week whether the workflow actually saves clinician time. That speed of signal is hard to replicate elsewhere.
Reimbursement For Digital Therapeutics: The Hardest Path
This is the “hard mode,” but it’s getting less hypothetical. In the U.S., reimbursement typically requires (a) the product to be treated as a regulated clinical intervention (often FDA-cleared/approved when applicable), and (b) the workflow to fit existing billing pathways.
Two useful signposts:
- The APA has summarized emerging reimbursement pathways for digital therapeutics, including new codes approved by CMS for certain digital mental health interventions.
- Medicare has also recognized FDA-cleared prescription digital behavioral therapy via HCPCS coding (e.g., A9291).
Practical reality check:
- Coverage varies by payer, and “having a code” doesn’t guarantee payment at a rate that makes your unit economics work.
- The clinical evidence bar is real. A reimbursable digital therapeutic typically requires randomized controlled trials, FDA clearance, and ongoing real-world performance data.
- Time to revenue is measured in years, not months. This is a long-term moat strategy, not a way to fund the next 12 months.
- If you’re not aiming for FDA-cleared DTx, reimbursement is usually not your first monetization lever. Employer licensing or hybrid subscription tends to be faster.
Reimbursement is the highest-moat model once you achieve it, and the easiest to underestimate before you do. Most teams should treat it as a long arc, not a starting point.
Which Monetization Model Fits Your Product?
A simple way to sanity-check the fit:
| Your Situation | Most Likely Model | Why |
|---|---|---|
| Therapist practice or group practice | Provider/practice SaaS or freemium plus human | Buyer and user incentives align; fast feedback loop |
| Consumer-facing wellness app | Freemium plus paid (human or premium AI) | Low friction first step, paid tier monetizes engaged users |
| Employer wellness or EAP-adjacent | B2B PMPM licensing | Clear procurement channel, mature buying behavior |
| Clinical product with strong evidence | Reimbursement (long-term) plus B2B (near-term) | Reimbursement is the moat; B2B funds the journey |
| Multi-stakeholder clinical platform | Combination of provider SaaS + B2B | Practices buy workflow value, employers/payers buy outcomes |
Two patterns worth internalizing:
- The strongest products usually run two monetization models in parallel, not one. A B2B employer contract pairs naturally with a freemium consumer funnel; a provider SaaS pairs naturally with a long-term reimbursement strategy.
- The model you can win in the next 12 months matters more than the model you’d love to be running in 5 years. Pick the model that gets your product in front of real users now, and let revenue (not roadmap slides) tell you what to build next.
How to Measure Mental Health Chatbot ROI
If you can’t measure the ROI of your mental health chatbot, you can’t defend it: not to your CEO, not to a B2B buyer, not to the clinical leadership who has to vouch for it. The good news is that ROI for a mental health chatbot is measurable in 2026. The harder part is picking the right metrics for your product, and not drowning in vanity numbers along the way.
Start With What You’re Actually Trying to Improve
ROI measurement breaks down the moment you try to optimize for everything at once. Pick the two or three outcomes that matter most for your specific product, and design your measurement plan around them.
Common primary outcomes by product type:
- Therapist practice or clinic SaaS: clinician time saved per client, no-show rate, intake-to-first-session time, between-session engagement.
- Employer wellness: utilization rate, employee-reported wellbeing, EAP referral rate, downstream healthcare cost trend.
- Consumer freemium: activation rate, retention at week 4 and week 12, free-to-paid conversion, average revenue per user.
- Reimbursable digital therapeutic: clinical outcomes (PHQ-9, GAD-7, symptom-specific scales), adherence to protocol, real-world performance.
The trap to avoid: tracking “engagement” as a primary metric without tying it to an outcome. Engagement is a leading indicator. ROI is what engagement translates into.
The Core Metrics Categories
Most mental health chatbot ROI analyses pull from four metric categories. The right balance depends on your buyer and your product, but a defensible measurement plan touches all four.
Engagement and adoption. Activation rate, weekly active users, average session length, conversation completion rate, retention curves at 4 and 12 weeks. These are leading indicators: high engagement enables outcomes, but engagement alone isn’t ROI.
Clinical and wellbeing outcomes. Validated symptom scales (PHQ-9, GAD-7, WHO-5), self-reported wellbeing, sleep quality, completion of evidence-based modules (CBT, mindfulness). For products in regulated workflows or with clinical claims, these are non-negotiable.
Operational outcomes. Clinician time saved per client, intake-to-first-session time, no-show and late-cancellation rates, support ticket deflection, escalation accuracy (true positives vs. false positives in your safety routing). These translate directly into dollars for B2B buyers.
Financial outcomes. Cost per active user, conversion rate (free to paid, AI to human), customer acquisition cost, lifetime value, downstream healthcare cost trend (for employer and payer buyers). The further down this list you go, the longer the time horizon.
A Simple ROI Framework You Can Actually Use
For most products, a useful ROI framework looks like this:
- Inputs. All-in cost of running the chatbot: build amortization, infrastructure, LLM costs, clinical content review, safety operations, customer success, compliance overhead.
- Time savings. Clinician minutes saved per client per week, multiplied by clinician hourly cost and number of clients.
- Quality improvements. Better intake, faster triage, fewer no-shows, higher completion of homework and exercises. These translate into either revenue (more clients served) or cost avoidance (fewer wasted slots).
- Outcomes value. For B2B and payer contexts: improved symptoms, fewer escalations to higher-cost care, better employee productivity. For consumer: higher retention and conversion.
- Risk-adjusted ROI. Subtract the cost of safety incidents, compliance issues, and brand-damaging events. A single significant incident can wipe out a year of efficiency gains.
The honest framing: the strongest ROI cases for mental health chatbots in 2026 come from operational and quality improvements (intake, triage, between-session continuity, no-show reduction), not from “we replaced a clinician.” The replacement framing is rarely true and almost always sells short the actual value.
What Buyers Actually Want to See
Different buyers care about different parts of the ROI story. Tailoring the conversation matters.
- Therapist practice owners want: clinician time saved per week, no-show rate, client retention, ease of clinical review.
- Employer wellness buyers want: utilization, employee satisfaction, EAP referral patterns, and signals of downstream healthcare cost impact.
- Health plans and payers want: clinical outcomes, member engagement, cost-of-care trend, and evidence quality.
- Consumer investors and operators want: activation, retention curves, conversion, ARPU, and CAC payback.
- Clinical leadership wants: safety incident rates, escalation accuracy, evidence base for clinical content, and audit-readiness.
If your dashboard can answer all five views without rebuilding from scratch, you’re in good shape.
Common ROI Measurement Mistakes to Avoid
- Cherry-picking timeframes. A 2-week clinical outcomes win is interesting; a 6-month one is meaningful. Don’t oversell short-term data as long-term proof.
- Ignoring the safety side of the ledger. A chatbot that saves clinician time but produces unsafe responses isn’t ROI-positive. It’s a liability waiting to surface.
- Counting non-incremental engagement. If the people using the bot would have engaged with care anyway, you haven’t moved the access needle. Compare against a control or a pre-launch baseline.
- Confusing activity with outcomes. “Users sent 1.4M messages this quarter” isn’t ROI. “Users who completed 4+ CBT sessions saw a 4-point PHQ-9 improvement” is.
- Not tracking the cost side. Many teams track usage and outcomes but never reconcile against actual operating cost, which makes the ROI calculation impossible to defend in a board meeting.
A useful gut-check: if you handed your ROI dashboard to a skeptical CFO and a skeptical clinician, would both of them sign off on the math? If only one of them would, the dashboard isn’t ready.
If you want to discuss your therapeutic chatbot idea with a company that prioritizes your business’s growth besides product development, contact us here.
[This blog was originally published on 8/31/2022 and has been updated for more recent content]
Frequently Asked Questions
What is a mental health chatbot?
A mental health chatbot is an AI-powered conversational program that provides mental health support, psychoeducation, self-assessment, mood tracking, and structured coping exercises through text or voice. It is not a replacement for a clinician. The strongest products are explicit about that boundary and route users to human support whenever the situation calls for clinical judgment.
What tools do you recommend for creating a chatbot?
It depends on the conversation type and your hosting constraints. For structured clinical flows, Dialogflow CX or Rasa are still strong choices. For open-ended AI-led conversations, hosted LLM APIs from OpenAI, Anthropic, or Google are the practical default in 2026. On top of either, you should layer a runtime guardrails framework (NeMo Guardrails, Guardrails AI, or an in-house validator) plus a vector database (Pinecone, Weaviate, pgvector) for retrieval-augmented generation over your approved clinical content.
How long does it take to develop a mental health chatbot?
A focused MVP can ship in roughly 12 weeks (3 months) if scope is tight (one workflow, basic escalation, minimal integrations). Production-ready builds with stronger safety, analytics, and multi-channel support typically take 6 to 9 months. Enterprise clinical builds with FDA-pathway considerations run 12 to 18 months or longer.
What platforms work best for mental health chatbots?
Mobile-first (native app or mobile web) is usually the best starting point. Web portals are common for employer and clinic rollouts and admin workflows. Messaging channels (WhatsApp, Messenger, SMS) can be great in markets where users already live in chat. Treat messaging as an add-on, not the foundation.
How much does it cost to build a mental health chatbot MVP?
For an MVP, plan on $30,000 to $80,000. To stay in that range, keep the scope tight: one target user group, one primary workflow (intake plus routing, or between-session support), a minimal UI, basic escalation logic, and minimal data retention. Costs jump when you add EHR integrations, therapist scheduling and billing, messaging or video, multi-state rollout requirements, or deeper reporting and admin workflows. More advanced AI-led builds typically run $80,000 to $150,000+, and enterprise clinical builds often start at $200,000+.
Is ChatGPT HIPAA compliant for therapy apps?
By itself, no. HIPAA compliance is an end-to-end system property: infrastructure, access controls, logging, encryption, retention and deletion, vendor contracts (including BAAs), and how you handle transcripts and identifiers. If you use an LLM in a therapy app, treat it as one component inside a HIPAA-ready architecture and only send the minimum necessary data. Always confirm whether your LLM or API vendor will sign a BAA for your use case before any PHI is involved.
How do I get FDA clearance for a mental health app?
Start by defining intended use and claims. FDA oversight is driven by what you claim the software does (diagnose, treat, prevent, mitigate) and how it functions. If you are in digital therapeutic / SaMD territory, expect to build a Quality Management System, run verification and validation, and produce evidence proportional to risk (often including clinical evaluation). Many teams begin with a regulatory positioning memo and a pre-submission strategy before committing to the full pathway.
What is the best AI model for a mental health chatbot?
There is no universal “best.” Choose based on safety controls, consistency, latency, cost, and how well the model behaves inside your guardrails. For mental health use cases, what matters most is your safety architecture (escalation logic, restricted response modes, runtime validation, and output validators), plus your testing process across edge cases. Most teams prototype with more than one frontier model (GPT-4o, Claude, Gemini) and select the final option based on measured performance in their specific workflows and risk scenarios. For data residency or enterprise constraints, self-hosted open-weight models (Llama 3, Mistral) are worth evaluating, but they trade convenience for significantly more engineering load.