
More than 1 billion people worldwide live with a mental health condition right now, and the supply side isn’t catching up. Therapist waitlists run weeks to months, crisis lines stay stretched, and primary care isn’t built to absorb the overflow. That’s where mental health apps land, and that’s the category we’ve been building into for the better part of a decade.
This guide is what we’d hand a founder or PM walking into mental health applications development cold. What types of apps are getting funded right now, what HIPAA-compliant looks like beyond the BAA checkbox, real cost ranges from projects we’ve shipped, and the specific traps that turn a 6-month build into 14 months. If you’re developing an app for mental health and have a therapist or clinician on the team, even better. Most of what’s in our portfolio came out of those conversations.
Table of Contents:
- Mental Health Applications Development Market Overview
- Types Of Mental Health Applications
- Must-Have Mental Health App Features
- Results You Get from Creating a Mental Health App
- Monetization Strategies for Mental Health Applications
- Key Aspects of Mental Health App Development
- Mental Health App Development Best Practices
- Step-by-Step Guide on How to Create a Mental Health App
- Step 1: Choose the target audience and platforms
- Step 2: List possible features and run rapid prototyping
- Step 3: Code the solution for patients and doctors
- Step 4: Test your app
- Step 5: Release and keep updating the app
- Tech Stack for Mental Health Apps
- 10 Takeaways from Negative Reviews on Mental Health Apps
- Top Concerns Mental Health Applications Need to Handle
- Key Challenges in Mental Health App Development
- Mental Health App Development Cost
- Future of Mental Health App Development
- Topflight’s Experience with Mental Health App Development
Mental health applications development market overview
Mental health stopped being a wellness niche
Developing an app for mental health is no longer a niche category. More than 1 billion people worldwide live with a mental health disorder, with anxiety and depression at the top of the list. The supply side keeps failing the same way: appointments are weeks out and care doesn’t stick between sessions. That’s the gap.
Mental health app projects fit that gap directly. A patient who’d wait three weeks for a therapy slot can open an app today and get a CBT module, journaling prompts, a peer-support thread, or async messaging with a clinician. For founders, that mix of unmet need and growing reimbursement is rare in digital health. Developing an app for mental health is one of the few categories where you can hit a public-health number and still run a real P&L.
The clinical receipts are finally landing. In March 2025, Dartmouth published the first randomized controlled trial of a generative AI therapy chatbot. 210 adults with major depressive disorder, generalized anxiety disorder, or eating-disorder risk got 8 weeks with Therabot or a waitlist:
- depression symptoms dropped 51%
- anxiety reduced by 31%
- eating-disorder body-image concerns dropped 19%
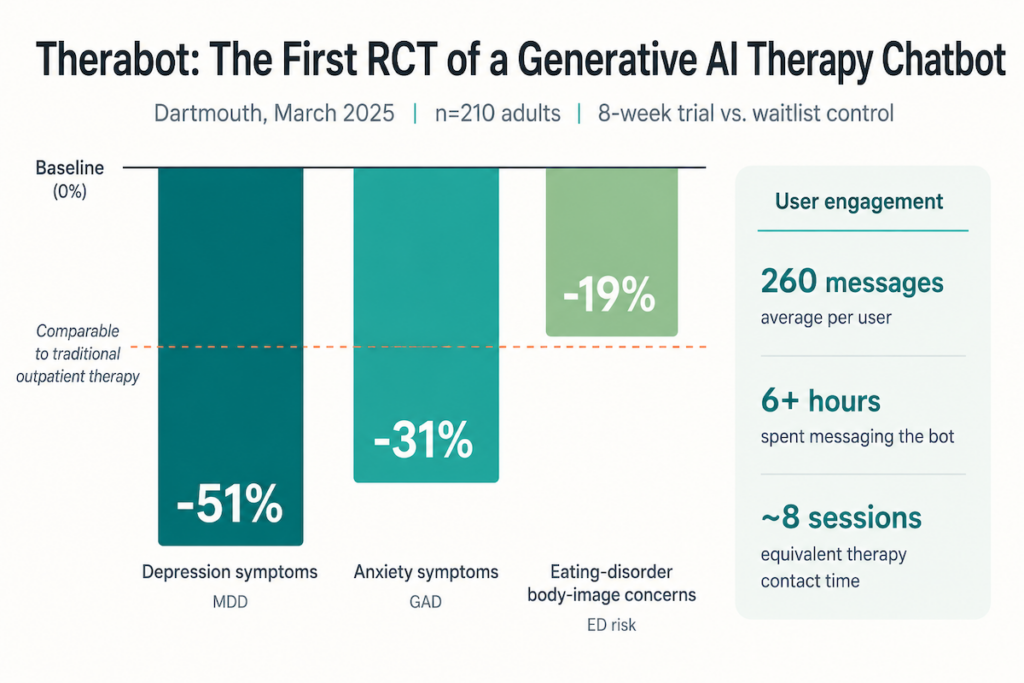 The average user sent 260 messages and spent over 6 hours messaging the bot, roughly 8 therapy sessions worth of contact. Dartmouth called the improvements comparable to traditional outpatient therapy. That’s the highest evidence bar the category has cleared.
The average user sent 260 messages and spent over 6 hours messaging the bot, roughly 8 therapy sessions worth of contact. Dartmouth called the improvements comparable to traditional outpatient therapy. That’s the highest evidence bar the category has cleared.
On the system side, these tools are getting woven into crisis care pathways, youth mental health programs, overdose prevention initiatives, and broader behavioral health services. The “consumer wellness” framing is dated. As more counseling apps get evaluated and integrated into actual care delivery, they stop being side projects and start looking like infrastructure.
Mental health is one of digital health’s recurring funding theses
Zoom out to the broader digital mental health category (apps plus enterprise behavioral platforms, clinician marketplaces, and employer benefits) and the market is forecast to grow from about $27.8 billion in 2024 to more than $153 billion by 2034.
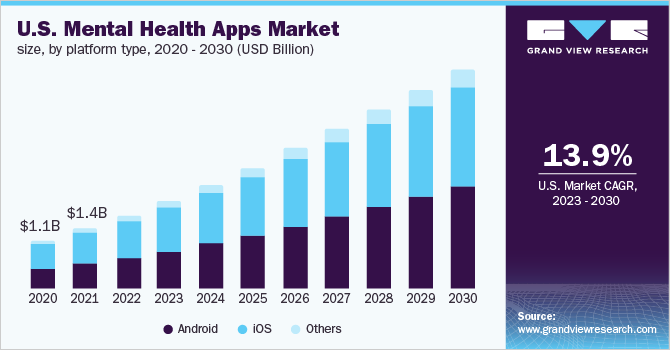 Image credit: Grand View Research (all rights belong to Grand View Research, Inc.)
Image credit: Grand View Research (all rights belong to Grand View Research, Inc.)
Funding tells the same story. In 2023, digital behavioral health companies raised about $1.2 billion across 65 deals, and youth mental health startups grew their share of behavioral health dollars from 15% in 2018 to 34% in 2023. U.S. digital health overall pulled in $6.4 billion in H1 2025, up from $6.0 billion in H1 2024. Investors are still writing checks even as the broader market normalizes post-pandemic, and mental health became one of the recurring theses in those portfolios.
COVID-era urgency was supposed to be the driver, but app usage stayed elevated long after the pandemic surge. Reimbursement experiments and enterprise contracts replaced the early tailwind, and the “therapy uberization” trend (on-demand access and async support) is sticking around. What changed in 2026 is the bar. Today the win condition is clinical credibility and real integration with care delivery. Launching an app doesn’t make you a player anymore.
The payer side is moving too. In November 2024, CMS approved three new reimbursement codes for FDA-cleared digital therapeutics covering Medicare patients. In September 2025, Cigna became the first major commercial insurer to follow, announcing it would start covering FDA-approved digital therapeutics. The Medicare codes only reach the small set of devices that cleared FDA. For that set, the business model stopped being subscriptions alone. If you’re building toward an FDA submission, the path to reimbursement is now less hypothetical than the path to a working product.
Five numbers worth holding onto before you build
- About 10,000 smartphone mental health apps sit in major app stores. New apps appear and disappear constantly, so the visible market churns month to month.
- Most of those apps have no clinical evidence behind them. A 2025 review found only ~15% of general mental health apps have any feasibility or efficacy study, and earlier work pegs the share with strong research support at <2%.
- More than 70% of people worldwide who need mental health care still don’t receive adequate treatment, and mobile apps are one of the few realistic ways to reach users with support for depression, anxiety, and suicidality risk.
- Adverse-event reporting is bad. A 2024 systematic review found that only 55 of 171 trials involving mental health apps reported adverse events at all. That’s why safety monitoring and escalation paths have to be built in from day one, not retrofitted after the first incident.
- Between 2011 and 2030, the global economic output loss from mental disorders is projected at $16.3 trillion. The case for digital mental health infrastructure isn’t a 5-year story.

The bar moved in 2025 because regulators finally noticed.
- August: 44 state attorneys general sent a formal letter to Google, Meta, and OpenAI demanding safer chatbot products for minors.
- September: the FTC opened a formal inquiry into the same companies, and APA testified before the Senate Judiciary Committee urging Congress to make it illegal for any chatbot to pose as a licensed professional.
- By November, APA had issued its first formal health advisory stating that engagement with GenAI chatbots and wellness apps for mental health can “have unintended effects and even harm mental health.”
- In January 2026, Character.AI settled multiple lawsuits brought by parents of teens who died by suicide or attempted self-harm after extended chatbot use.
Table stakes for any consumer-facing mental health app shipping in 2026: pre-deployment safety testing, real crisis pathways, age-appropriate gating, and no AI-as-therapist framing without licensure. Companies that built to that bar from day one are about to look smart.
Why mental health app development pencils out
Why build a mental health app at all? Four forces line up in this category that rarely line up elsewhere in digital health: demand outstrips supply for mental health applications, reimbursement is finally catching up, product value compounds with engagement, and the regulatory bar is high enough to create real defensibility for whoever clears it. Most digital-health categories have one or two of those. Mental health has all four.
| Reason | Why it matters in practice |
|---|---|
| Accessibility | Apps clear the geography and scheduling barriers that knock people out of care before they start. The reach goes deepest in rural counties and underserved zip codes, where the nearest in-network psychiatrist can be hours away. |
| Cost economics | Per-user economics improve as you load more users onto the same backend, which is why nearly every consumer mental health app moved to subscription pricing early. The marginal cost per active user keeps dropping past the break-even point; clinic models can’t match that curve. |
| Privacy by default | Stigma keeps a real share of people out of therapy. An app is private by default: no building to walk into, no clinician’s office hours to schedule around, no explaining to a partner where you’re going on Wednesday nights. That privacy reaches the population that wasn’t seeking care in the first place, which is half the unmet-need story. |
| Personalization that earns its keep | ML lets you do things at the user level that clinicians can’t do across thousands of patients: spotting when a check-in pattern shifts, or routing someone to a clinician when their PHQ-9 score crosses a threshold. That personalization is what keeps people in the app past week 3, where most consumer health apps lose them. |
| Engagement signal as a moat | Engagement signals tell you which interventions are actually working and where users are churning. Healthcare apps that ignore this signal layer get out-iterated by ones that don’t, and the gap compounds over years. |
Now to the types of apps actually getting built.
Types of mental health applications
Mental health apps don’t fall into one bucket. The seven categories below cover what’s actually getting built and funded in 2026, and each carries a different clinical scope and regulatory load. The lines blur in practice. A peer-support app that adds CBT modules becomes a CBT-plus-community app, and most teletherapy platforms ship with self-management features built in.
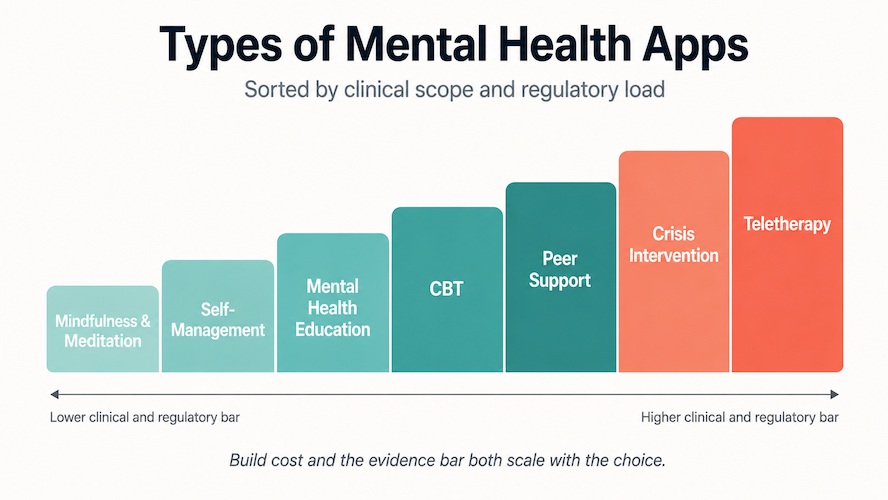
If you’re planning to start a mental health app, the most useful first question is which combination of these categories you actually want to ship, and how clinical you’re willing to go. Self-management and meditation are the lowest-regulation entry points; teletherapy and crisis intervention sit at the highest end. Build cost and the evidence bar both scale with that choice.
Most of these categories push every serious build into custom mobile applications development once clinical workflows and compliance enter the picture.
Self-management apps
Self-management apps are the daily driver of digital mental health: mood trackers, journaling tools, habit builders, and self-reflection prompts that help users notice what’s going on long before they show up in crisis.
These apps typically let people:
- log moods, activities, and triggers over time
- connect patterns between sleep, work, relationships, stress, and anxiety
- set micro-goals like “take a walk when stress hits 7/10”
- get coaching nudges between therapy sessions
They’re also the category most founders instinctively want to build first, usually as a pretty chart. “Year in Pixels” aesthetics are the easy part. The harder build is data a clinician or coach can actually use in a session.
![]()
Evidence backing varies a lot across the category:
- popular mood-diary apps like Daylio have usability and acceptability studies behind them (easy to use, users keep coming back)
- multi-tool self-help apps like Sanvello layer CBT content and have been evaluated in randomized and naturalistic trials for anxiety and depression
- newer self-discovery apps like Breeze combine mood tracking with CBT-flavored courses, but so far rely mostly on expert design and user feedback rather than formal clinical research
If you’re developing a mental health application in this space, the opportunity is to wire self-tracking directly into a therapist’s notes or a PCP’s chart. Apps that ship insights into a clinical workflow get used past month two. Dashboards that sit in isolation get deleted by month three.
The serious version of this category is a symptom tracker that captures PHQ-9, GAD-7, sleep, energy, and medication adherence at the right intervals, then routes the data to whoever owns the user’s care. That’s a different build than a streak counter, and the cost-of-care use case is what opens up payer or enterprise distribution.
Related: How to Build a Chatbot
Example self-management apps
| App | Primary use case | Clinical evidence level* | Platforms | Monetization |
|---|---|---|---|---|
| Sanvello | Self-guided CBT for anxiety and depression with journaling and mindfulness modules | High: evaluated in multiple clinical and naturalistic studies for anxiety/stress reduction | iOS, Android | Freemium + paid subscription; some payer/enterprise coverage |
| Daylio | Micro-diary and mood tracker for building self-awareness around daily habits and mood patterns | Moderate: usability and experience studies support effectiveness in use, but no large RCTs | iOS, Android | Freemium with premium subscription |
| Breeze | Self-discovery app that combines mood tracking with short CBT-flavored courses | Low: CBT-inspired content and therapist endorsements, no published clinical trials yet | iOS, Android | Freemium with in-app purchases / subscription |
*Evidence level is a qualitative summary based on published studies and systematic reviews, not a formal grading system.
Cognitive behavioral therapy (CBT) apps
CBT apps take what used to live in a workbook or a 50-minute session and turn it into structured exercises you can do from a phone. A real CBT app gives you:
- thought records and cognitive restructuring
- exposure ladders and behavioral experiments
- worry time and structured problem-solving for stress and anxiety
For founders, CBT apps sit closer to “digital therapeutics” than to generic wellness or meditation apps. They’re also the category most scrutinized by clinicians and payers. CBT has a long track record in the literature, and people expect the digital version to respect that.
 Typical CBT apps help users:
Typical CBT apps help users:
- learn core CBT concepts (automatic thoughts, cognitive distortions, avoidance, and behavioral activation)
- complete short, guided exercises tied to specific problems (panic, social anxiety, insomnia, etc.)
- track progress over time with symptom scales and goals
- sometimes blend in coaching or live-therapist access
Evidence varies a lot across the category leaders:
- MindShift CBT (by Anxiety Canada) has multiple studies showing reductions in anxiety and depressive symptoms over 4–16 weeks of use.
- Wysa has RCTs and service evaluations across depression, anxiety, chronic pain, and healthcare-worker stress, plus work on therapeutic alliance with an AI coach.
- Bloom is a self-guided “video CBT” app with strong product traction. Its evidence base draws on the broader self-guided CBT literature, with limited Bloom-specific trials so far.
If you’re creating a mental health application in this category, the 2026 expectations are clear lineage to evidence, guardrails for users with active suicidality, and a build that’s more than a worksheet with push notifications. Clinical review teams catch the CBT-ish stuff fast now.
Example CBT apps
| App | Primary use case | Clinical evidence level* | Platforms | Monetization |
|---|---|---|---|---|
| MindShift CBT | CBT-based self-help for anxiety, panic, worry, and related depression symptoms | High: multiple studies (including 16-week trials) report reductions in anxiety/depression and improved quality of life | iOS, Android | Free; funded by Anxiety Canada / grants |
| Wysa | AI-guided CBT coaching with tools for anxiety, depression, stress, and chronic pain | High: RCTs and evaluations show symptom reductions and acceptable therapeutic alliance in multiple populations | iOS, Android, Web | Freemium; B2B/B2B2C employer and health-system deals |
| Bloom | Self-guided “video CBT” sessions for stress, anxiety, mood, and habit change | Moderate: grounded in CBT with supportive evidence for self-guided CBT generally; limited Bloom-specific published trials to date | iOS, Android | Subscription (monthly/annual), sometimes via partners |
Mindfulness and meditation apps
Mindfulness and meditation apps are the gateway drug of digital mental health. They’re low-friction and low-stigma, and for a lot of users they’re the first mental health tool that ever lives on the home screen.
They typically help users:
- reduce stress and anxiety with short guided sessions
- improve sleep with evening practices and “sleep stories”
- build a basic meditation habit through streaks and content playlists
 The category already cleared two product proofs that most mental health categories haven’t:
The category already cleared two product proofs that most mental health categories haven’t:
- it monetizes well (B2C subscriptions plus employer-plan deals)
- it shows up in real trials with measurable improvements on sleep disturbance and on depression/anxiety symptoms
The research is past the “does any of this work?” stage. The current questions are which dose, which content, and for which audience. Recent meta-analyses show mindfulness apps can acutely reduce depression and anxiety, with researchers calling out the need for longer-term, higher-quality trials.
Google Play sorts this category into a wide range, from light-touch meditation apps with breathing exercises and habit trackers on one end, to clinically-anchored programs targeting sleep or panic on the other. Users don’t draw those lines as cleanly. They open whatever they hope will make them feel a bit better today. If you’re building a meditation app in 2026, your real competition is whatever else is on the home screen at 11pm when a user can’t sleep.
You may also be interested: How to Make a Meditation App Like Headspace
Example mindfulness and meditation apps
| App | Primary use case | Clinical evidence level* | Platforms | Monetization |
|---|---|---|---|---|
| Headspace | Guided mindfulness and meditation for stress, anxiety, focus, and general well-being | High: multiple randomized and controlled studies report improvements in stress, depression, anxiety, and work-related outcomes across various populations | iOS, Android, Web | Subscription (consumer) + employer/health-plan partnerships |
| Calm | Mindfulness and sleep-focused meditation to improve sleep quality and emotional health | High: RCTs show improvements in sleep-related symptoms and fatigue, plus reductions in depression and anxiety among adults with sleep disturbance | iOS, Android | Freemium; premium subscription; B2B enterprise offerings |
| Insight Timer | Large library of free guided meditations and timers for stress, anxiety, and sleep | Moderate: used in intervention studies and observational research on anxiety and stress; strong engagement data | iOS, Android | Freemium; premium subscription |
Peer support apps
Peer support apps sit in the middle ground between therapy and social media: moderated communities, anonymous support groups, shared journaling spaces, and “lived-experience” forums where people talk to others who’ve been through the same thing.
 This category matters for two reasons:
This category matters for two reasons:
- Teen and young-adult mental health. The demographic hardest to reach through traditional care prefers peer-to-peer environments over clinics.
- Chronic conditions. Diabetes, chronic pain, addiction, ADHD, and long-COVID communities cluster in these apps because traditional care doesn’t offer continuous emotional support.
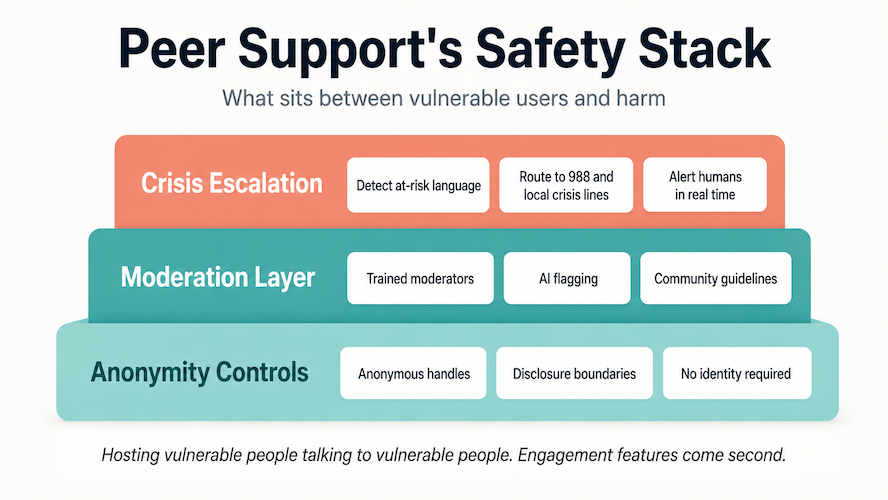
Scale matters less in this category than founders assume. Safety is the real differentiator:
- moderation standards
- crisis escalation rules
- anonymity controls
- community guidelines trained into both humans and algorithms
If you’re developing a mental health application in this category, the product risk is simple. You’re hosting vulnerable people talking to vulnerable people. Guardrails matter here more than engagement features.
Example peer support apps
| App | Primary use case | Clinical evidence level* | Platforms | Monetization |
|---|---|---|---|---|
| 7 Cups | Anonymous emotional support groups + volunteer listeners for anxiety, stress, and loneliness | Moderate: peer-support + listener model studied in multiple evaluations; good evidence for acceptability, limited data on clinical outcomes | iOS, Android, Web | Freemium; paid access to licensed therapists |
| Wisdo | Community-based peer groups for loneliness and life transitions, with guided group paths | Low to moderate: strong engagement data; limited independent research; some studies on loneliness reduction but no large-scale RCTs | iOS, Android | Subscription; some employer/plan reimbursement |
| HeyPeers | Certified peer-support meetings for addiction recovery, anxiety, grief, and chronic conditions; often used by nonprofits and treatment programs | High: tied to standardized peer-support models with evidence for improved functioning; platform itself has program-level evaluations | Web, iOS, Android | Pay-per-meeting + subscriptions; org partnerships |
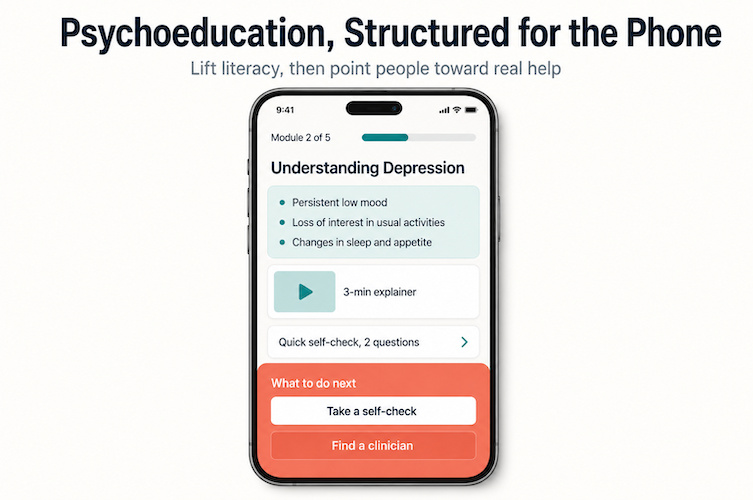
Mental health education apps
Mental health education apps are basically asynchronous psychoeducation with better UX: structured content, short videos, interactive diagrams, and self-checks that explain what’s happening and what to do next. The target users range from individual patients and parents to entire workforces.
 They matter because:
They matter because:
- most people hit Google before they hit a clinician
- clinicians don’t have time to deliver full psychoeducation in every session
- health systems, schools, employers, and insurance plans want standardized, vetted mental health content they can roll out widely
A good education app lifts mental health literacy and reduces stigma, so users show up to a first therapy or coaching session already knowing what’s on the table. Recent reviews of web/app-based mental health literacy interventions show meaningful gains in knowledge and help-seeking attitudes when the content is structured and evidence-based. If you’re creating an app for mental health in this category, that gain is your real KPI.
Example mental health education apps
| App | Primary use case | Clinical evidence level* | Platforms | Monetization |
|---|---|---|---|---|
| MindPublic | Open-access mental health literacy for teens and adults: core concepts, stigma reduction, how to get help, and how to read mental-health information critically | Low to moderate: grounded in established mental health literacy frameworks; no app-specific trials yet, but aligns with evidence that structured web/app MHL programs improve knowledge and attitudes | Android | Free; no ads, no in-app purchases |
| Baby Comfort Guide | Psychoeducational guide for parents of 0–24-month-olds with crying, sleeping, feeding, or settling problems; combines expert info, videos, diary, emergency plans, and self-care tips | High: randomized controlled trial shows reduced parenting stress and increased knowledge vs. waitlist, with positive implementation feedback; now rolled out as a free public app | iOS, Android | Free; funded by academic and regional public-health initiatives |
| UN’s MindCompanion | Mental health literacy and self-assessment for UN peacekeepers and staff: explains common issues and teaches coping skills, with the goal of encouraging formal help-seeking | Low to moderate: designed as part of a broader UN mental-health strategy; described in UN manuals as an education-and-care tool but no published RCTs yet | iOS, Android | Free; provided by the United Nations as part of internal mental-health support |
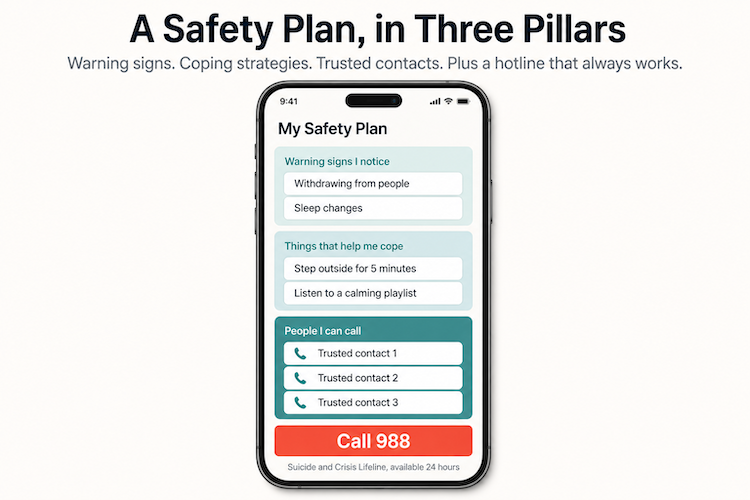
Crisis intervention apps
Crisis intervention apps live at the sharp end of digital mental health. They’re built for the worst few minutes of someone’s week: suicidal ideation, or a panic spike that won’t break.
Typical functions include:
- Personalized safety plans (warning signs, coping moves, support contacts, and reasons-to-live the user has pre-decided)
- Tap-to-call / tap-to-text access to crisis lines (988 in the US, equivalent local lines elsewhere, plus a saved trusted contact)
- Resource directories tailored to region and situation
- Guidance for supporters and clinicians on how to respond in a crisis
For founders, the metrics here are latency to a working contact and reliability when the path fails. Liability exposure follows from those two. If your app sits in the critical path between a user and help, you inherit obligations around:
- uptime and failover for the contact paths (what happens if crisis line numbers change?)
- routing to local resources where the user actually is
- clear messaging that the app does not replace emergency services
- audit trails for the calls and texts initiated through your app
On the evidence side:
- The Stay Alive app (Grassroots Suicide Prevention, UK) has independent evaluations: a 4-year review found 76% of at-risk users reported the app helped them stay safe, with high satisfaction and meaningful stigma reductions across the cohort.
- Apps like MY3 focus on safety planning, with warning signs, coping strategies, support contacts, and reasons-for-living as the core inputs. The app itself doesn’t have RCTs, but the underlying planning framework is well-evidenced.
- Suicide Safe, built on SAMHSA’s SAFE-T framework, targets clinicians rather than the public. It turns an evidence-based assessment protocol into a mobile reference and decision-support tool.
If you’re designing a mental health app with any crisis-focused functionality, the bar is simple: never ship a shiny UI on top of an unreliable safety net.
Example crisis intervention apps
| App | Primary use case | Clinical evidence level* | Platforms | Monetization |
|---|---|---|---|---|
| Stay Alive | Suicide-prevention app providing a safety plan, grounding exercises, quick access to crisis lines, and resources for supporters of people at risk | High: independent evaluations (2020–2024) report 76% of at-risk users stayed safe and significant reductions in stigma; widely deployed in UK public-health campaigns | iOS, Android | Free; funded by charity and public-sector partners |
| MY3 | Personal safety-plan app where users define three key contacts, warning signs, coping strategies, and resources to reach out to when suicidal thoughts appear | Moderate: strongly aligned with evidence-based safety-planning interventions; app itself has implementation and program-level evaluations but limited formal trials | iOS, Android | Free; supported by suicide-prevention organizations |
| Suicide Safe (SAMHSA) | Clinical decision-support app for providers based on the SAFE-T 5-step suicide assessment and triage framework; offers guidance on risk assessment, clinical interview moves, documentation, and referral pathways | Moderate: built directly on an established, evidence-based clinical guideline (SAFE-T); app-specific research is limited, but the underlying protocol is widely endorsed | iOS, Android | Free; U.S. federal public-health resource |
Teletherapy applications
Teletherapy apps are where “mental health app” stops being a nice-to-have and starts competing with brick-and-mortar clinics. These platforms connect people with licensed clinicians and wrap scheduling, messaging, billing, and clinical documentation around the encounter.
 The headcount of “therapy apps” out there doesn’t tell you much; the category definitions are fuzzy. The questions worth asking about a real teletherapy platform are:
The headcount of “therapy apps” out there doesn’t tell you much; the category definitions are fuzzy. The questions worth asking about a real teletherapy platform are:
- Does the platform handle licensure geography, supervision requirements, scope-of-practice rules, and the differences across the 50 states?
- Can it support multi-state care without becoming a compliance grenade?
- Is there any proof it delivers better access or measurable outcomes than a phone number on a clinic website?
That’s the bar you’re competing against. Many of the platforms that now dominate best telemedicine apps lists already bundle dedicated mental health services, which means your edge has to come from deeper clinical workflows or a sharper niche. A new logo on top of “video visits for therapy” gets you nowhere in 2026, especially given that telemedicine app development cost already starts in six figures before you factor in clinical operations.
The structured end of the category is a marketplace model that wraps real clinicians around familiar product mechanics. A measurement-based-care dashboard, between-session homework, clear referral paths from the app to a higher level of care, and outcome reporting back to payers are the table stakes for any platform competing with the established players. If you’re creating an app for mental health in the teletherapy lane, every UX mechanic should make the clinical work easier for both sides of the screen.
Related: Telemedicine App Development: Everything You Need to Know
Example teletherapy applications
| App | Primary use case | Clinical evidence level* | Platforms | Monetization |
|---|---|---|---|---|
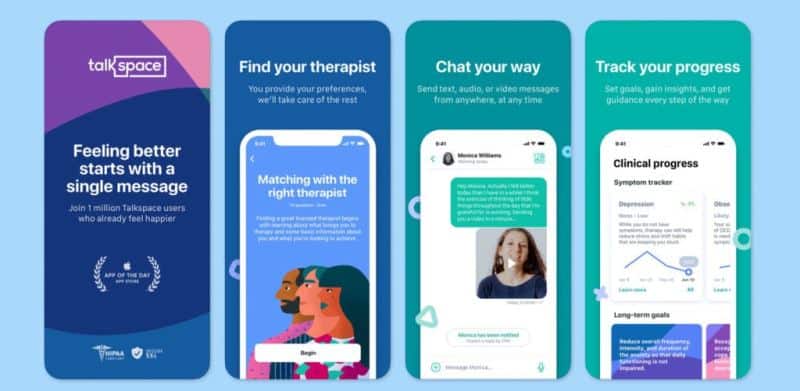
| Talkspace | Large-scale teletherapy and psychiatry platform offering text-based and live-session formats (audio/video) with licensed clinicians; strong focus on employer and health-plan contracts | High: multiple studies and real-world analyses report reductions in depression and anxiety symptoms and workplace-related distress in users receiving Talkspace interventions compared to usual care or baseline; growing body of outcomes data in employer populations | iOS, Android, Web | Subscription-based packages; employer and health-plan reimbursement; some EAP integrations |
| BetterHelp | Direct-to-consumer and employer-offered online therapy marketplace connecting users with licensed therapists for asynchronous chat or live phone/video sessions | Moderate: the underlying teletherapy model is well supported in the literature; BetterHelp-specific published data focuses mainly on satisfaction and symptom reduction in observational cohorts rather than large RCTs, but still shows meaningful improvement for depression and anxiety over time | iOS, Android, Web | Monthly subscription; some employer and payer partnerships |
| SonderMind | U.S.-focused network that matches patients with in-network therapists (virtual and in-person), emphasizing insurance coverage, measurement-based care, clinician support tools, and outcome reporting back to payers | Moderate to high: built on teletherapy and measurement-based care models with strong evidence; emerging program-level data on improved access and engagement, though fewer app-specific trials than long-standing DTC players | iOS, Android, Web | Insurance-based reimbursement (commercial + some public plans), co-pays; limited DTC self-pay options |
Therapy application types at a glance
You can think of teletherapy apps as a cluster of related subtypes:
- Synchronous teletherapy (video/audio): digital replacement for the traditional 50-minute session
- Asynchronous therapy (chat-first): ongoing written or audio exchanges; higher frequency, lower intensity
- Therapist marketplaces: discovery and matching layer that can plug into external EMRs or practice-management systems
- Therapist companion tools: scheduling, documentation, outcome measures, and homework delivered alongside sessions
- Blended-care platforms: therapy + coaching + digital programs + medication management in one care model
Most serious products blend at least two of these. The “type” you pick determines your regulatory overhead, clinical staffing model, and payer story more than your UI design ever will.
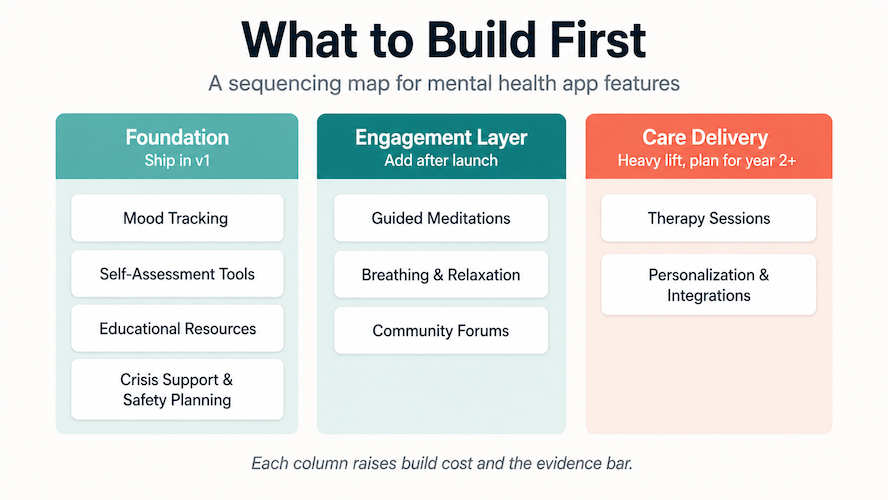
Must-have mental health app features
The right feature set turns a generic product into a mental wellness app that people actually use, and that clinicians can trust. The 9 features below are the building blocks worth thinking through early when you’re designing a mental health app. Skip too many and you ship a journal with a streak counter. Try to build all 9 in v1 and you ship in 14 months instead of 6.
Mood tracking
Mood tracking is still the backbone of most consumer-facing builds:
- quick emotional check-ins
- simple tags for triggers or contexts
The trick is to make logging nearly invisible and surface insights in a clean dashboard that filters signal from noise. If you want to go deeper on the visualization layer, check out how to build a dashboard web app and apply those principles to symptom and behavior data.
Guided meditations
Guided meditations anchor the daily routine around short, repeatable practices. Pair breathing or mindfulness sessions with medication reminders and sleep logging so you’re reinforcing context-aware habits. Even a single well-timed nudge (“breathe before you open email”) can shift a user’s perceived stress over the course of a week.
Self-assessment tools
Self-assessment tools make your app feel useful from the first session by giving users a quick sense of “where am I today?”. Well-designed self-assessment features blend clinically recognized scales like PHQ-9 and GAD-7 with conversational interfaces, like avatar-based chatbots in the style of Sensely that walk people through check-ins.
You can layer in gamified assessment modules that connect cognitive skills training with early risk flags, turning a feature-light app into something clinicians can use between visits.
For a deeper technical dive into this space, start with our Machine Learning App Development Guide.
Therapy sessions
If you’re serious about building a teletherapy app or a telemedicine mental health app, the bar is a stable, low-friction virtual therapy experience that doesn’t feel like a bad Zoom clone. That means:
- letting patients book appointments in a couple of taps
- handling time zones gracefully
- supporting secure messaging plus high-quality video for live sessions
On the clinician side, session notes, outcomes data, scheduling, and billing should live in one place. Providers shouldn’t have to juggle four tabs to get through an hour of patient work, and any mental health app project that ignores this ships into a non-adopting market.
For extending support beyond the session, see our take on Medical Chatbots: The Future of The Healthcare Industry.
Educational resources
Educational resources turn your product into more than a symptom dial by helping people understand what they’re dealing with. That might include plain-language explanations of what a mental health disorder is, how bipolar disorder presents differently from attention problems, or why schizophrenia needs a different care path than burnout.
You can also fold in practical modules on diet, sleep hygiene, exercise patterns, and early warning signs of relapse. Knowing when to escalate matters as much as knowing how to cope.
Need inspiration? Our guide on How to Build an Education App shares ways to turn passive content into active learning experiences.
Breathing exercises and relaxation techniques
Breathwork and micro-relaxation tools are tiny interventions with outsized impact, especially when they’re wired to data. Connecting short practices to a sleep tracker lets you time interventions based on sleep patterns and daytime fatigue signals. A short guided relaxation exercise can become the bridge between “I’m overwhelmed” and deeper therapeutic engagement, especially for users who aren’t ready to commit to full sessions yet.
Community forums
Community features turn your product from a tool into a place. Carefully-designed structured channels work better than an unstructured feed:
- topic channels
- small groups for specific conditions
- anonymous posting for sensitive shares
A well-built community reduces stigma around topics that get hidden elsewhere, like LGBTQ youth experiences or addiction recovery. The build needs serious moderation and clear mental health disclaimers. Engagement signal in this category comes from structured contributions and resolved help-requests; surface metrics like likes don’t move outcomes.
Crisis support and safety planning
For higher-acuity populations, you want a basic crisis layer: safety plans, one-tap hotline access (988 in the US, equivalent local lines elsewhere), and a visible escalation path to emergency services. The layer matters because people in distress will use whatever tool is in front of them. Your job is to make sure that tool routes them somewhere safe and fast.
Personalization and integrations
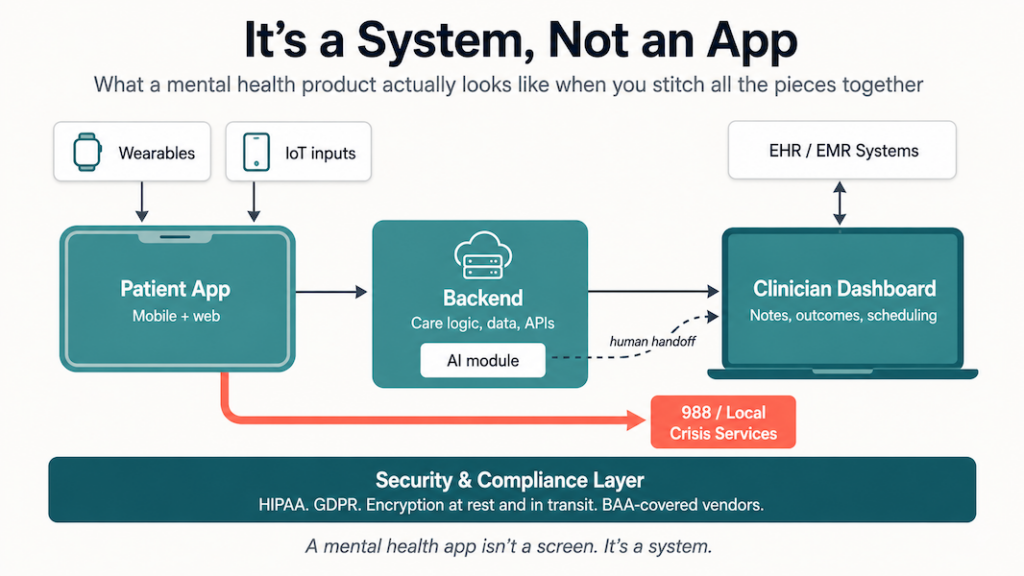
The features above get dramatically more valuable when they’re stitched together: personalized routines configured by the user, clinician-configured care protocols, and integrations with calendars, wearables, EHRs, and clinical decision-support systems.
That’s where the app moves from “nice mental health app” to a product that supports care teams. Good personalization respects the constraints around it: clinical workflows, compliance requirements, the limits of the underlying tech stack, and the user’s limited attention budget. Being clever doesn’t beat being usable inside a 5-minute session window.
Results you get from creating a mental health app
When founders evaluate the possible results of developing an app for mental health, the conversation usually centers on impact: who gets helped, how fast, and at what cost. Digital mental health tools work alongside traditional therapy as an extension layer, absorbing cases the in-person system can’t reach in time. The COVID-19 surge made that clear, when demand spiked past clinic capacity for two years running.
The outcomes below are where well-built mental health apps move the needle in production. Each one shows up in real metrics: utilization, cost-per-user, retention curves, and clinician hours saved.
Mental health support reaches people clinics can’t
Instant access is the biggest gain. A mental health specialist can support a user without a clinic visit, on the user’s schedule. Patients dealing with minor but acute issues (heartbreak, anxiety spikes, early relapse signals) can get meaningful support through online therapies or AI-guided check-ins before things escalate.
Learn more about artificial intelligence nursing burnout and its role in supporting mental health professionals.
For users who carry stigma around seeking help, digital entry points feel safer. They can start with an AI bot or a self-help module, then escalate to human clinicians only when needed. That single shift gets people engaging early, when intervention is more useful.
The cost economics beat face-to-face therapy
Digital platforms reduce the financial barrier that keeps many people out of care. Compared to face-to-face therapy, mobile mental health applications typically offer:
- lower session costs at the consumer-pay tier
- flexible chat-based or asynchronous models that don’t require a 50-minute time block
- targeted self-help modules for anxiety management or low-acuity emotional crises
- employer-sponsored access via EAP or health-plan rails
This is also why healthcare app development services surged during the pandemic. Digital care offered an affordable stopgap when traditional therapy wasn’t accessible, and continues to do so for millions today.
Personalized care that in-person visits can’t deliver
One of the underrated advantages of mental health apps is that users control their own data. They can review their mood history, track medication consistency, and see how symptoms evolve over months. Periodic in-person visits don’t capture that kind of longitudinal signal.
This creates a more personalized care experience for users and clinicians both. Users build better self-understanding; clinicians come into sessions with richer longitudinal data. AI-driven micro-interventions add another layer by adjusting exercises or recommendations to real-time inputs.
The challenge is getting these personalization features to evidence-based status, which takes significant clinical research and a multi-year roadmap. When that work pays off, personalization becomes a strategic moat.
Learn about fitness mobile app development in our dedicated blog.
Less pressure on traditional healthcare systems
Digital tools act as a buffer for overloaded health systems. When patients can self-manage between sessions by reviewing psychoeducation, practicing coping skills, tracking symptoms, and following medication adherence, they rely less on urgent visits and crisis-level escalations.
These tools also free clinicians to spend more time on high-acuity cases by absorbing the routine check-ins for milder issues. The system-level result is reduced operational burden, particularly in regions where mental health professionals are scarce.
Challenges around user trust, tech literacy, and confidentiality are real and need engineering attention. The upside is also clear: digital mental health solutions absorb volume that clinical systems can’t sustainably handle, and they let the traditional care layer focus on what only humans can do.
Monetization strategies for mental health applications
Most founders who develop a mental health application start with the same short list of monetization options available for mobile apps. Not all of them make sense for products that deal with vulnerable users and regulated care. The work here is picking models that fit clinical value and user trust, beyond whatever your favorite consumer app does.

Paid premium version
The classic one-time “paid app” still works in narrow cases: tightly scoped tools with clear outcomes and a well-defined niche (a specialist assessment or a clinician utility, for example).
- The upside is simplicity and fewer billing surprises
- The downside is that you cap lifetime value on day one
If you go this route, nudge serious buyers toward a web checkout to avoid platform fees and gain more control over invoicing and refunds.
In-app purchases
In-app purchases are underused in mental health. Beyond the paywall-everything approach, you can sell structured programs and premium content bundles on top of a solid free baseline. This works well for self-management or CBT-style apps where users buy specific modules as they progress (the “social anxiety pack” pattern), without committing to a full subscription on day one.
Mobile ads
You can run a mental health app on an advertising model, but you need to be ruthless about how. Full-screen ads and jarring placements between crisis screens are a fast way to destroy user trust and end up in App Store review hell.
If you use sponsors at all, think low-key banners in clearly non-clinical areas (gratitude journaling, generic wellness content). Anything related to diagnoses, prescriptions, or insurance has to stay firewalled from ad targeting completely.
Subscription
Look at the top-performing mental health apps and you’ll see a pattern: nearly all of them lean on a subscription model. The behavior fits: these apps deliver ongoing support and content that evolves with the user’s care journey. The subscription revenue model lets you trade one-off purchases for predictable ARR, which investors and acquirers actually care about.
The basics still matter: transparent pricing and easy cancellation, plus a clear reason to keep paying past month three. That reason usually comes from new programs unlocking, clinician touchpoints, or outcome-tracking that surfaces user progress over time. Whenever possible, steer users to subscribe via web so you’re not giving away 30% margin to the app stores forever.
Freemium
Freemium remains the most defensible way to grow: a serious free tier that delivers real mental-health value, plus a paid layer that adds depth like richer analytics and clinician-connected features. The key is avoiding “crippleware.” Free users should genuinely benefit, and the paid layer should deliver more than cosmetic upgrades. In mental health specifically, the freemium line often falls between self-guided content and anything that touches live humans, care teams, or longitudinal data.
Enterprise and payer contracts
For many clinical-grade products, the real money sits with enterprise buyers: employers, health plans, and health systems. The monetization model looks different in that world:
- PMPM (per-member-per-month) contracts
- bundled pricing around outcomes like reduced burnout or lower PHQ-9 scores
- integrations into existing care-management or EAP programs
This path takes longer to validate but tends to produce higher retention and tighter coupling to clinical outcomes.
Whichever models you pick, the throughline is simple: in mental health, monetization only works if users, clinicians, and regulators still trust you in a year. Pricing is flexible; trust is not.
Key aspects of mental health app development
Before you commit to sprints and Gantt charts, map out what makes a mental health app actually work. The job covers clinical fit and emotional UX before you even get to the commercial model that pays for all of it. Below is the rest of the starter kit, broken down by build phase, with a focus on the parts most founders skip when they’re learning how to build a mental health app.

Research and planning
Teenagers dealing with social anxiety. Veterans coping with PTSD. Therapists managing burnout. Postpartum parents in the first 90 days. Each group brings wildly different expectations. Start by narrowing your scope. Who are you building for, and what outcomes do they want?
Spending real time here before creating a mental health application saves you from expensive pivots later. You’ll be building against validated needs from week one.
- Run surveys and 1:1 interviews to define use cases
- Study Reddit threads and 1-star app reviews from competitors
- The killer question is why users quit their current mental health app
Get clinical advisors involved early. Otherwise you risk building a glorified to-do list app with a meditation sticker slapped on it.
You’ve already read about subscriptions and freemium models. Now think beyond user payments:
- Partner with employers for EAP integrations
- Explore partnerships with digital clinics or payers
- Build a CPT-coded tool and work toward reimbursement eligibility
Just avoid surprise paywalls. Nothing erodes trust faster than offering help and then hiding it behind a checkout screen mid-crisis.
Design and user experience
Mental health apps aren’t productivity tools. Users may be in distress, distracted, or one tap away from closing your app forever. So design for clarity and calm:
- Use muted tones and readable fonts with generous touch targets
- Avoid unnecessary animations and gamification unless they serve a therapeutic goal
- Localize content and diversify visuals so the app feels inclusive
- Test layouts in dark mode and high-contrast accessibility settings
Interactive check-ins, mood tracking streaks, audio-guided mindfulness sessions, and short reflection prompts land harder than a “level-up” badge does in this context.
Core features
Not every mental health app needs mood tracking, AI chatbots, journaling whiteboards, and social features baked in. Focus on one “core job” (supporting recovery, guiding CBT, or 24/7 therapist access) and build around that core.
One core feature that works beats ten that kinda do.
Development and security
Cross-platform is often the fastest way to market (React Native or Flutter are solid picks). If you’re leaning into AI, you’ll want Python for the backend and secure GPU-ready infrastructure. Planning for EMR integrations? FHIR support, OAuth2 for patient auth, and HIPAA-safe cloud services like AWS or GCP are the table stakes.
Avoid shiny-object syndrome. Choose tools that scale with you and keep development cycles lean.
Compliance is the non-negotiable layer. If you handle PHI, you’re bound by HIPAA in the US and possibly GDPR elsewhere. Encrypt everything at rest and in transit, and bake in access controls from day one. Firebase and Airtable don’t belong anywhere near anything remotely clinical.
Better yet, work with vendors who offer signed BAAs and compliance out-of-the-box.
Testing and deployment
Ship fast, but don’t break trust. Beyond functional testing, mental health apps benefit from:
- Usability testing with neurodiverse users
- Clinical review of content and flow
- Data privacy audits
- Pre-launch penetration testing of any AI or ML components
If users report confusion or hesitation in feedback, take it as a harm signal. Mental health users notice friction differently than productivity-app users do.
Post-launch maintenance
Mental health content and clinical practices evolve. Your app needs to keep up. Quarterly releases, rotating therapeutic content, and ongoing vulnerability testing are baseline maintenance for this category.
Once you have users relying on your product for their emotional wellbeing, every feature you ship (or break) carries higher stakes than a typical consumer app. Treat your backlog like a care plan.
Mental health app development best practices
Here’s what makes a mental health app project hold up in practice. The step-by-step on how to develop a mental health app is next.
Consumer-centric design
From the app logo through onboarding to the main screens, design is your primary tool for credibility and trust. Designing a mental health app is about signaling that the user is safe here, and that signal lives in onboarding tone and in how the app handles bad days.
- Is onboarding smooth and short?
- Can a new user tell what the app does within 10 seconds of opening it?
- Does the UX match what people already do on iOS or Android?
Answer those honestly and you’ll know whether the app earns a second session. Keep the palette restrained on both ends: oversaturated colors and washed-out neutrals can both put off someone who’s already feeling low.
Read our guide to Healthcare App Design
Also read: How to build a Pharma App: The Ultimate Guide
Security
Health data is sensitive, so users care a lot about how you protect it. Take security seriously from day one, the way you would with any other healthcare app.
HIPAA is the baseline. Add a privacy policy users can actually read, education on safe practices, and GDPR compliance if you operate in the EU. Local rules apply wherever you ship.
And keep a runbook for security incidents on file before you need one.
Doctor-centric back end
Therapists need their own surface too. Picture a web or mobile app for talking with patients, plus a separate dashboard that tracks symptoms and progress over time. The back end is half the build.
Multi-platform support
Users typically jump between phone and laptop in a single day, with a tablet or smartwatch in the mix for the more device-heavy ones. The app should follow them across these surfaces, even if you can’t ship every one on day one. Pick the two with the highest projected session counts and start there.
Internet of medical things
Wearables and smartphones give you a real-time view of physical activity and sleep patterns. A drop-off in either usually shows up days before the patient mentions it in session. That’s actionable data for the treatment plan.
Also Read: IoT App Development Guide
Interoperability
Mental health data should move cleanly from your app into the other psychiatry systems therapists already work in, like EHR/EMR. That’s where the next partnership conversations start: payers and integrated care groups.
Related: EMR/EHR System Development Guide
Cautious use of AI
AI can make or break a mental health app. You can’t train your healthcare machine learning algorithms on live patients, and you need a clean human handoff every time the model gets out of its depth. We’ve seen AI engines recommend a glass of bourbon to relax.

Psychiatric emergency
Tell users plainly that this app isn’t designed for emergencies (God forbid, suicide attempts), and put the right hotline numbers in front of them anyway. Keep the emergency surface tight: maybe a single call button and an optional alert to a family contact. Don’t promise emergency messaging unless you can staff it 24/7 with real humans.
Apply these and you’ve laid the groundwork to develop a mental health application that holds up in practice. Now the actual step-by-step on how to build a mental health app.
Step-by-step guide on how to create a mental health app
Now the actual process of how to build a mental health app, step by step.
Each step below has a real decision attached. Skip one and the next gets harder.
| Step | Description | Key actions |
|---|---|---|
| Step 1: Define audience | Identify your target users and platforms for the app. |
|
| Step 2: Plan features | List and test potential app features using prototypes. |
|
| Step 3: Start coding | Develop the app with a focus on technical and compliance needs. |
|
| Step 4: Test | Ensure the app is fully functional and meets quality standards. | conduct functional, performance, security, and other tests |
| Step 5: Launch & improve | Release the app and continuously update it based on feedback. |
|
| Each step below expands on the row above. | ||
Step 1: Choose the target audience and platforms
Whether you’re aiming at seniors or teenagers will shape your platform mix. Knowing your patient cohort early lets you design experiences that actually land. Research moves to cover when making a mental health app:
- identify the age group your app aims to help
- scan competitors for what your audience already expects
- prepare a typical patient profile
Ideally, a few patients from your target audience will participate in the next step and help you narrow the UX/UI of the solution.
Step 2: List possible features and run rapid prototyping
When it comes to custom developing an app, listing features and testing them with a prototype lets you verify design ideas before you spend on code.
Prototyping first cuts cost by an order of magnitude compared to jumping straight into product development, and it shortens how long it takes to build your app. You get to validate the business idea with zero coding, which is the most expensive part of mental health software development.
Bring developers in at this stage too. They’ll flag the designs that look fine in Figma and break in implementation.
If you want to skip Figma entirely, use a no-code prototyping tool with stock interface elements and have test users review the result on their own phones.

Step 3: Code the solution for patients and doctors
This is where most of your development time goes. We recommend Agile with interim tests every iteration. Practical moves for keeping the timeline honest:
- Use third-party HIPAA-compliant audio/video calling SDKs if you’re building a telemedicine therapy app
- Use other off-the-shelf components, like a chat with audio messages, to expedite delivery
- Set up the DevOps pipeline so developers aren’t spending sprint time on environment work
- Follow cybersecurity best practices according to HIPAA regulations
At Topflight, we’ve always worked to lower the tech barrier (and lower the cost with it) by reusing available components. Over the years we’ve built up a library of ready-to-use modules for authentication, appointment scheduling, chat, secure messaging, and other prerequisites common to most mental health applications.
Read our guide on how to find and hire mobile app developers
Related: HIPAA Compliant App Development: The Ultimate Guide
Step 4: Test
Testing runs through every iteration, but this step is the big pre-release sweep. Cover at least:
- Functional testing
- Performance testing
- Compatibility testing
- Interface testing
- Unit testing
- Stress testing
- Security testing
Related: Mobile App Testing: Methods, Best Practices, Tools and More
Step 5: Release and keep updating
Once the app’s been thoroughly tested, it’s ready for users. A round of app store submission tremors (less so if you’re working with pros), and the app is out, ideally with a mobile marketing campaign behind it.
Then you switch into post-launch mode. Track in-app analytics, address user requests, fix issues as they surface, and ship updates on a steady rhythm. A clean DevOps setup keeps maintenance costs from creeping.
If you added Google Analytics or a similar service during development, the live app will feed you engagement data that drives the next round of updates and points to growth areas you didn’t see in research.
Working through these steps gives you a real path to a mental health applications development project that holds up in the market.
Tech stack for mental health apps
Most modern stacks work for a mental health applications development project. The decisions that actually matter come down to:
- platform reach (iOS, Android, web, or all three)
- on-device ML or AR/VR needs
- integration count with EHR, CRM, payments, and video SDKs
Pick on those. Framework choice is downstream.
For a cross-platform play, React Native or Flutter cover iOS and Android from a single codebase and let you extend to web later with shared logic. Security on either framework comes from the libraries and managed services you wire in (encryption, KMS, BAA-covered hosting). Don’t let anyone tell you the framework itself carries it.
Native mobile technologies, e.g. Swift for iOS and Kotlin for Android make sense if you plan to add on-device machine learning or use advanced platform features like AR/VR.
On the server side, Node.js with a managed cloud (AWS, GCP, or Azure) is a solid default. Plan integrations up front. If your CRM has an out-of-the-box API for app data, use it. If not, you’re building one, and that’s a real line item.
| Layer | Recommended option(s) | When to prefer it | Key trade-offs | Mental health-specific notes |
|---|---|---|---|---|
| Client app (mobile) | React Native or Flutter (cross-platform) | • You need iOS + Android from day one – Fast MVP with a small team and shared UI logic |
• Slightly heavier bundles and some perf tuning for complex UIs – Platform-specific edge cases still exist |
• Good default for most mental health MVPs – Easier to keep release cadence in sync across platforms – Add native modules later for video, sensors, or encryption |
| Client app (mobile) | Swift (iOS) / Kotlin (Android) | • You need top-tier UX or AR/VR – Heavy on-device ML (e.g., offline sentiment or risk models) – You have separate iOS/Android teams |
• Two codebases, two pipelines – Higher cost of change and maintenance |
• Best for products that are “mobile-first clinical tools” – Easier to use OS-level security and biometrics |
| Web client | React / Next.js, Angular, or Vue | • You’re building therapist dashboards or admin consoles – Need responsive web for payers and employers – SEO matters for patient acquisition |
• More surface area to secure (web + mobile) – Browser compatibility issues to test |
• Ideal for provider portals and care-team views – Use role-based access to separate patient and clinician UX – Easier to plug into EHR or CRM back office |
| Backend (API + business logic) | Node.js (TypeScript) on AWS / GCP / Azure | • Real-time features (chat, presence, notifications) – High-concurrency teletherapy sessions – Team already knows JS/TS |
• Needs disciplined architecture to avoid “callback soup” – CPU-heavy ML better offloaded to separate services |
• Strong fit for chat, room management, scheduling – Use managed services with HIPAA-eligible SKUs only – Make audit logging and consent flows first-class features – Push CPU-heavy ML off the main API onto dedicated workers |
| Backend (API + business logic) | Python (FastAPI / Django) with ML services | • You’re leaning into AI/ML triage, recommendations, or NLP – Data-science team is Python-first – Need tight coupling between models and clinical logic |
• Less ideal for very chatty, real-time workloads – Requires strong DevOps to scale cleanly |
• Good for risk-scoring, summarization, and personalization engines – Keep PHI out of non-compliant third-party LLM APIs – Log every model decision that touches safety or clinical routing |
| Database | PostgreSQL or MySQL (managed), plus Redis for caching | • Need relational data with reporting, billing, and audit trails – Want managed backups and encryption |
• Schema changes must be planned – Requires tuning for very large event streams |
• Store PHI only in encrypted, HIPAA-eligible instances – Separate analytics data from raw PHI where possible – Design for right-to-erasure and export from day one |
| Infrastructure & DevOps | AWS / GCP / Azure with IaC (Terraform, CloudFormation) | • Need HIPAA-aligned building blocks – Expect audits, BAAs, and security reviews – Multi-region uptime for teletherapy |
• Cloud misconfigurations are the main risk – Over-engineering is easy if you copy big-tech patterns blindly |
• Insist on BAA coverage before storing PHI – Centralize logging and monitoring for incident response – Automate security patching and vulnerability scans |
| Integrations | EHR/EMR (FHIR / HL7), CRM, Payments, Video SDKs | • Need clinician workflow integration (Epic, Cerner) – Want automated billing and compliant video |
• Vendor APIs can be brittle and slow to change – Each new integration adds support overhead |
• Wrap integrations behind an integration layer or middleware – Treat every external system as a potential PHI boundary – Predefine what happens when an integration is down during a session – Track API change logs for the vendors you depend on |
| Analytics & Observability | Mixpanel/Amplitude + OpenTelemetry + SIEM | • You care about engagement, retention, and funnel analytics – Need audit trails for security and compliance – Want to test product changes safely |
• Risk of leaking PHI into logs or third-party tools – Over-instrumentation can hurt performance |
• Keep PHI out of analytics events by design – Monitor drop-offs around high-risk flows (assessments, crisis) – Use logs to prove you handled safety-critical events correctly |
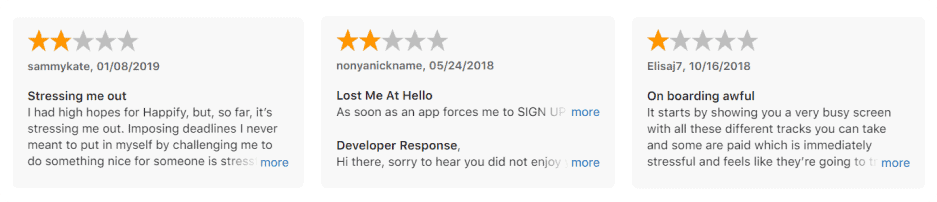
10 takeaways from negative reviews on mental health apps
Learning how to create a mental health app that doesn’t earn one-star reviews starts with reading the one-star reviews. We’ve watched the same 10 complaints surface in mental health app reviews for years. The patterns below are the ones worth designing around.
- Test every login path end to end. Facebook, Google, and Apple sign-in can each break in subtle ways that show up first in one-star reviews.
- Make every UX element earn its place. If users can’t tell why they earn points, they stop chasing them within a week.
- Find the balance between upselling a subscription and giving value first. The reviews you don’t want all sound the same: tricked into paying.
- Design has to signal safety. A mental health app that looks clinical-cold or commercial-pushy turns people away in equal measure.
- Onboarding decides whether you get a second session. Every extra screen between download and first useful moment costs users.
- Keep security from getting in the way of ordinary use. A 2FA flow that locks people out at the wrong moment ends in uninstall.
- Be clear about pricing, renewal terms, and how to cancel. Back it up with support that responds same-day.
- Triage bugs by impact on the therapeutic loop. A crash mid-journal entry costs you more than a layout glitch.
- Support the latest mobile OS and the screen sizes your patients actually use.
- Ship new content on a rhythm. Long-time users notice when the same exercises keep cycling, and engagement drops.
Top concerns mental health applications need to handle
Trust gets built in the privacy details
Users are about to hand you their personal information, which means trust has to be earned through specifics: a privacy policy people can actually read, biometric authentication (fingerprint or Face ID), and an in-app knowledge base that answers the questions reviews keep raising.
Clinical evidence is the price of admission
People will check whether your app is backed by real research. If you don’t have published clinical evidence for what your app claims to do, you’re competing on vibes against apps that do.
The most evidence-backed apps often lose on engagement
We’ve noticed that the apps with the strongest scientific foundations often fail to deliver engaging day-to-day experiences. Rotating content on a rhythm, so users don’t see the same exercises week after week, is one of the fixes.
Copy and design can lower stigma or amplify it
A mental health app can take some of the edge off the social stigma around asking for psychological help, but only if the copy and design treat the act as ordinary. Clinical-sterile language amplifies the very stigma you’re trying to dissolve.
Plan around these concerns and you’ve laid the groundwork for how to build a mental health app that holds its place after install.
Key Challenges in Mental Health App Development
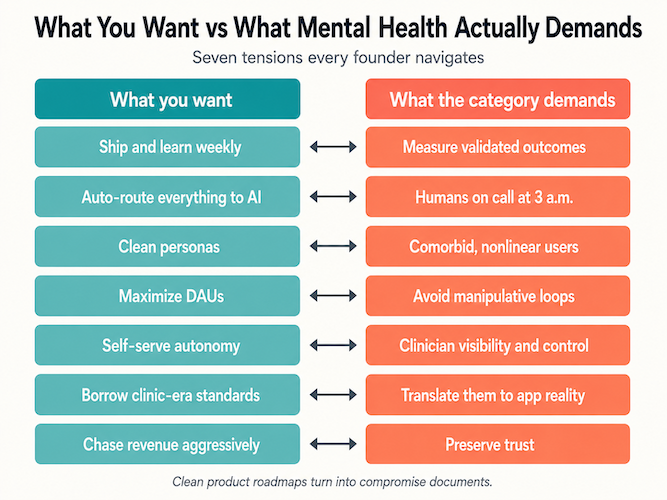
By this point you know what to build and roughly how to build it. The hard part is everything in between: the messy constraints that turn clean product roadmaps into compromise documents. Below are the friction points we hit on most mental health app development projects, in the order they tend to bite.
Validating the product without turning your startup into a research lab
Everyone says “be evidence-based.” Few teams have a concrete playbook for what that looks like with 18 months of runway and a half-built app.
The real tension:
- Clinicians and payers want validated instruments and defensible inclusion criteria
- Product teams want to ship and learn weekly
- Users just want something that helps them sleep or get through a panic spike
Bridging that gap usually means:
- picking a small set of outcomes you’ll actually measure (PHQ-9 or GAD-7 scores paired with retention data)
- designing features so they can be evaluated in the wild without breaking clinical integrity
Then accept that modest benefit plus solid retention in a real population is the working bar, and RCTs on toy features rarely survive contact with maintenance. You’re somewhere between a university lab and vibes-based care; walking that line is half the work.
Safety, escalation, and owning the “what if?” moments
Earlier sections covered crisis layers and safety planning. Once you build them in, you’ve accepted new responsibilities by implication. The questions that keep serious teams up at night sound like this: what happens if a user types explicit suicidal intent into a chat at 3:12 a.m., and what if the user is in a country where your hotline list is wrong or outdated?
You have to design three coordinated routes:
- technical (flags, queues, throttling, and audit trail)
- operational (who’s on call, what “urgent” actually means in your incident playbook)
- legal (what you commit to in the ToS versus what you actually do)
Writing “we are not an emergency service” into the ToS is the easy part. The hard part is making sure UX and backend do what the ToS claims they do, so a 3:12 a.m. flag actually surfaces to a human before sunrise.
Designing for people who don’t behave like personas
Personas are neat. Real users aren’t. They show up with overlapping diagnoses (anxiety with ADHD, or anxiety with substance use, more often than apps’ marketing pages admit). They show up with messy life constraints: shift work, caregiving, low digital literacy. And their motivation fluctuates week to week, sometimes day to day.
The UI work from earlier sections still stands. The deeper challenge is designing flows that work when people are exhausted or actively avoiding the very thing that would help them:
- paths that tolerate missed check-ins without punishing people
- copy that works for both the curious-and-stable user and the barely-holding-it-together user
- experiments that look at who drops out where, treated as a signal about your model of care rather than UX polish
Clinical reality is comorbid and nonlinear. Your product has to be usable in that world, not on the Figma board alone.
Engagement without dark patterns
You want retention. You’re not building Candy Crush. The challenge is keeping people engaged without:
- guilt-tripping them for missed streaks or spamming them with notifications at the worst moments
- using scarcity and FOMO tactics that would look terrible on the front page of a newspaper
Real engagement in mental health includes:
- whether people actually complete exercises that matter
- whether they come back after a lapse without feeling like they’ve “failed the app”
- whether usage correlates with real-world improvement, or only with the most gamified widget
- whether engagement holds past the first-month honeymoon
Strong habit loops and personalization, with the manipulative bits consumer apps lean on stripped out. It’s harder than it sounds, especially when growth and ethics disagree.
Balancing self-help autonomy with professional care
A big promise of mental health apps is that they let people do more on their own. The hard part is knowing when not to.
Some user journeys are safe to keep fully app-driven. Others need a human in the loop, and the design challenge is making that handoff feel like care all the way through, including the “you seem worse, upgrade to Pro therapy!” moments where the temptation to sound like a sales funnel is highest. Expectations also have to match what the product can actually do, which means a CBT bot shouldn’t be pitched as an alternative to trauma work or complex medication management.
The constant tension sits between:
- user autonomy
- clinician visibility and control
- regulator pressure on what you’re actually practicing here
Get that wrong and the product lands too clinical for casual users and too casual for clinicians. Neither audience commits.
Navigating standards that don’t quite fit apps yet
You’ve seen HIPAA, GDPR, and the laundry list of best practices already. Most mental health standards and guidelines were written for clinical settings, before app-based care existed as a category. That leaves awkward questions:
- How do you interpret “informed consent” when the first interaction is a 20-second onboarding carousel?
- What does “continuity of care” mean for a peer-support platform or a self-guided program?
- Which clinical frameworks do you anchor to (CBT, ACT, DBT, stepped care) when you’re not a licensed provider yourself?
You stitch four things together into a stack coherent enough for your medical advisors and your PM (with the legal team adding notes throughout):
- clinical guidelines
- digital-health regulatory expectations
- app-store policies
- internal ethics bars
Building a business without undermining trust
You’re shipping an app, and you’re building the company around it at the same time. That means:
- raising money in a market that has already burned through several mental-health hype cycles
- explaining to investors why the path to revenue doesn’t kill clinical integrity
- negotiating B2B2C deals (employers and payers) without turning users into engagement metrics in someone else’s slide deck
Every monetization decision (subscriptions, ads, enterprise contracts, B2B distribution) feeds back into the thing that keeps a mental health product alive: trust. You can refactor a tech stack. Trust with patients and clinicians takes much longer to rebuild than to lose.
Mental Health App Development Cost
The cost of developing a mental health app varies with project scope, app type, and how many platforms you support. A teletherapy app may start around $140,000. A simple mood-tracking app with self-monitoring features starts at around $70,000. These are MVP figures: what you launch with and build on from there.
If you’ve already researched telemedicine app development cost, expect serious mental-health builds to land in a similar band, with additional budget going into safety workflows, clinical integrations, and audit-ready data handling.
As with other mobile software, owners often forget the back end in the cost equation. You’ll need a database and an admin area for content management and configuration. Make sure quotes for your mental illness app cover all of that, including the parts that don’t show up in the demo.
| Scenario / app type | What the MVP typically includes | Platforms | Backend & admin scope | Typical MVP cost range (USD) | When this makes sense |
|---|---|---|---|---|---|
| Simple mood tracking app | • Daily mood check-ins and notes – Simple reminders plus basic charts showing patterns over time |
• 1 mobile platform (iOS or Android) – Optional responsive web view |
• Lightweight API – Secure database for user data – Minimal admin panel for content and config |
~ $70,000 (lean MVP starting point) |
• Testing a narrow use case – Validating demand and retention – Solo founders and small teams – Pre-investment proof of concept |
| Self-management / CBT tools app | • Mood and symptom tracking – CBT-style exercises and programs – Basic progress dashboards and goals – PHQ-9 or GAD-7 micro-assessments at intake |
• 1–2 mobile platforms (iOS + Android) – Web portal for content editing (optional) |
• API with role-based access – Content management plus basic analytics and audit logging |
~ $90,000 – $140,000 | • Direct-to-consumer launch – Early employer and school pilots – Preparing for future clinical studies |
| Teletherapy app (video + messaging) | • Secure chat, audio, and video sessions – Scheduling and availability management – Basic intake forms and notes for clinicians – Session billing and receipts for insurance reimbursement |
• iOS and Android – Web portal for therapists and admin |
• Full backend (users, sessions, payments) – Admin console for clinicians and support staff – Logging, monitoring, and basic reporting |
Starts around ~ $140,000 (grows with multi-region and complex features) |
• Clinics going virtual-first – Telehealth startups and branded provider groups |
| Crisis support / safety-plan app | • Safety planning workflows – Hotline and resource directory – Simple check-ins and risk signals |
• 1–2 mobile platforms – Web backend for updating resources |
• Secure storage of plans and contacts – Admin for content and hotline management – Region-aware configuration for resources – Audit trail for safety-plan changes and access |
~ $100,000 – $160,000 | • NGOs and public-health programs – Health systems extending suicide-prevention efforts – Research groups translating protocols into apps |
| Blended-care platform (therapy + programs + analytics) | • Teletherapy plus self-guided programs – Measurement-based care (PHQ-9, GAD-7, and similar instruments) – Multi-role access (patient, clinician, admin) |
• iOS, Android, and web – Integrations with external tools |
• Robust backend with multi-tenant support – Advanced admin and reporting – Integrations (EHR/EMR, payments, CRM) |
~ $200,000 – $350,000+ (depending on integrations and scale) |
• Venture-backed digital health startups – Provider groups or platforms targeting payers and employers at scale |
| Hidden cost drivers (all types) | • Multi-language support and accessibility (WCAG, screen readers) – Security hardening, audits, and compliance documentation – Analytics, experimentation, and feature-flag infrastructure – Customer support tools and internal admin workflows – Ongoing maintenance, OS updates, and library upgrades |
||||
Related Articles: Understanding App Development Costs, Healthcare App Development Costs
Future of mental health app development
The next decade of mental health apps comes down to whether your product behaves like infrastructure: clinically credible, evidence-backed, and able to sit inside real care pathways without spooking regulators.
From “app” to clinical infrastructure
Global digital mental health is on track to grow from roughly $24–28 billion in 2024–2025 to $80–150+ billion by the early 2030s, depending on whose forecast you read. That growth runs through a few specific channels:
- teletherapy platforms becoming standard benefits in employer and payer stacks
- digital therapeutics (Sleepio, etc.) getting NICE/FDA-style validation and reimbursement
- health systems plugging apps into intake, triage, and stepped-care workflows as primary tools, with budget and clinician hours behind them
Future winners will look like services that slot cleanly into payer and provider stacks, with APIs and real-world evidence behind the placement, plus governance documents ready for procurement review.
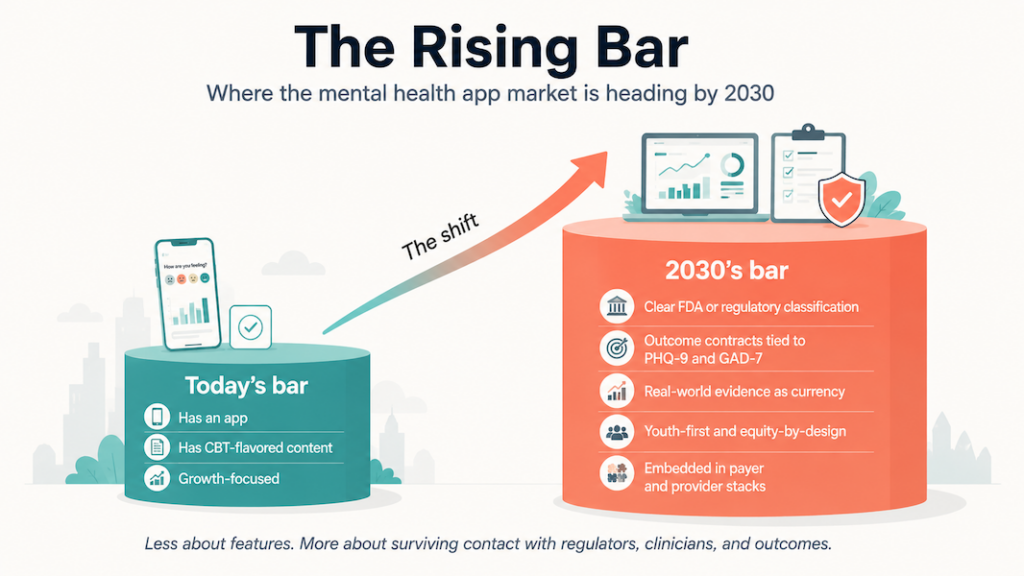
AI everywhere, finally regulated
The easy era of “just add a chatbot” is ending. Regulators are catching up:
- FDA has stood up a Digital Health Advisory Committee and is explicitly examining generative AI in mental-health-related devices and software
- U.S. states are starting to regulate AI therapy apps directly, with some banning AI-delivered therapy outright and others imposing disclosure and data-protection rules
If you’re betting on AI, the future looks like:
- clear lines between “wellness bot,” “clinical decision support,” and “software as a medical device”
- logged, explainable model behavior around risk and triage decisions
- audit trails that survive an OCR review with the AI-decision history intact
- marketing language that matches your true regulatory category, or you’ll get forced into one the hard way
The bar has moved to provably safe AI that’s correctly scoped to its regulatory category. Anything less reads to regulators (and increasingly to clinicians) as a liability waiting to happen.
Evidence and outcomes as the new currency
The market is crowded and user churn is high. Investors have already learned the “growth without outcomes” lesson the expensive way.
Over the next few years, expect:
- more NICE/FDA/insurer-style requirements for structured trials and real-world evidence
- outcome contracts where PHQ-9/GAD-7 score reductions drive payment, with session count as a secondary metric
- tighter expectations around safety data (adverse events, escalation performance, drop-off impact)
- patient-facing outcomes dashboards as a public commitment alongside internal analytics
The products that hold up will be built as if a clinical trial were already booked. Clean measures and clear cohorts get baked in early, with instrumentation that can answer “does this actually help?” alongside the usage analytics.
Youth, equity, and the digital determinants of mental health
WHO and others are now framing youth mental health in terms of digital determinants: how platforms and feeds shape risk and resilience, and how apps either compound or buffer those forces.
That pushes three things to the front of mental health app design:
- youth-first safety and consent flows that assume under-25s with heavy social-media exposure
- equity built into the spec from day one (language, bandwidth, device constraints, and cultural context as core requirements)
- policy alignment that lets governments and NGOs endorse the product inside national plans, with the procurement story prepared in advance
The bar is rising from “not obviously harmful” to “demonstrably helpful, especially for vulnerable groups.”
The future of mental health app development is about surviving contact with regulators and clinicians (real-world outcomes data is the arbiter now), while still shipping something people actually want to use. For founders, developing a mental health application will increasingly mean proving safety and measurable outcomes, with equity baked into the spec from day one, on top of the usual product-market fit story.
Topflight’s experience with mental health app development
We’ve seen upfront planning make or break mental health application development in practice, especially once real clinicians and patients start using the product.
Topflight’s experience in mental health app development covers several projects in the space. Four are worth walking through below.
Mi-Life: AI assistant for behavioral and developmental health
Mi-Life is one of our most technically demanding mental-health builds to date: a HIPAA-compliant AI-powered assistant designed for caregivers supporting individuals with developmental disabilities and Autism. The core challenge was cognitive overload. Staff were expected to memorize over 1,300 pages of client-specific protocols. Mi-Life turned that burden into a real-time, retrieval-augmented experience accessible by voice or text.

By combining GPT-4o, Azure AI Search, Whisper, and a RAG architecture, the app gives caregivers instant access to behavior plans, medication details, emergency steps, and shift-critical information, without exposing PHI during AI processing. The result is a tool that reduces medication errors and shortens onboarding while lowering caregiver mental strain.
On the engineering side, we implemented OTP-based authentication, role-based access controls, anti-hallucination safeguards, real-time scheduling, and a multi-tenant backend built for long-term expansion. The outcome: fewer incidents and higher staff satisfaction, with a replicable model for group homes and behavioral health organizations looking to modernize care.
Xzevn
We built a content recommendation engine that helped individuals maintain emotional health and improve their time management, decision-making, goal-setting, and self-improvement.
On the user-facing front, you’d input daily emotions via chatbot conversations, respond to daily questions, and like or dislike recommended articles and famous quotes. The app works as a personal diary that tracks mood changes, with no attempt at diagnosis. The treatment team sees those interactions through a connected admin web application.

The case study covers how our approach helped the client get into a business incubator.
Soberbuddy
Soberbuddy is a chatbot that helps people work through addiction recovery (alcohol and drugs). It guides users through evidence-based practices for relapse prevention: cognitive behavioral therapy and mind-body relaxation techniques.
Related Article: Addiction Recovery App Development
We inherited the project from a different team that had been overcomplicating things with unnecessary machine learning blocks, and the same team hadn’t found much traction in helping the client monetize the product. Since Topflight got involved, the project’s funding has reached $1.25m.

Since Topflight took it over, Soberbuddy has hit a 10% subscription rate, a 25% retention rate, and close to 100% activity. We’re still working on the app, layering in technologies that open up new treatment methods, like group therapy techniques.
The case study covers how to start a mental health app grounded in cognitive behavior therapy on the first go, with these numbers since we joined:
- Raised $1 million since the partnership started
- Lifted retention by 300%, with average engagement time up 40%
- Pushed app store rating from 3 to 4.5
- Grew user count to 30,000
- Cut cost of acquisition by 50%
Respirosa
Respirosa is a mindfulness app with a distinctive twist: users practice breathwork to their favorite music, with visual cues synced to the beat.
Users pick a tune by mood, genre, or artist and choose a color theme. The app pulls the song from Spotify and runs breathing sessions with an animation locked to the tempo. Projects like Respirosa also show how wellness app development can blur the line between “calm” consumer tools and clinically meaningful support, especially when breathing, music, and habit loops are wired into broader care programs.
Reach out if you want to develop a mental health app, or you want yours to outperform what’s already in the App Store.
Related Articles:
- A Guide to Building a Mental Health Chatbot
- Healthcare App Development Guide
- How to start a healthcare startup
- How to Create a Telehealth App
- How to collect healthcare data for your mobile apps
- Building Healthcare Apps that Improve Patient Data
- Artificial Intelligence in Healthcare
- How to build a doctor appointment app
- Wearable Technology in Healthcare
- Building Healthcare Chatbots
[This blog was originally published in September 2020 and has been updated for more recent data]
Frequently asked questions
How much does it cost to develop a mental health app?
$70,000 to $140,000 for a typical MVP, depending on the build. Bigger blended-care platforms can run $200,000 and up; [reach out](https://topflightapps.com/request-meeting/) for a quote tied to your specifics.
What tools should I consider to build a mental health app that relies on AI?
For an AI-powered mental health app today, look at LLM APIs (GPT-4o, Claude, Gemini), LangChain or LlamaIndex for orchestration, a vector store for RAG (Azure AI Search, Pinecone, or pgvector), and Whisper for voice. PyTorch still earns a spot for custom-trained models.
Do I need to provide any certificates to list my mental health solution in app stores?
Not at the moment.
How long does it take to build an average mental health tracker app?
4 to 6 months for a HIPAA-grade MVP. A pure wellness tracker without PHI handling can ship in 3 months, but most mental health apps cross into HIPAA territory fast.
Does my mental fitness app need to be HIPAA compliant?
If it stores any protected health information, yes.
How do I build a mental wellness app that's engaging and personal?
Use AI frameworks and a chatbot that learns from discussions with patients.