
You’ve got a health app that needs data out of Epic. Maybe it’s a clinician-facing tool pulling labs and medications, maybe it’s a patient app wiring into MyChart. Before you scope it, know one thing: “integrate with Epic” isn’t a single task. What you’re signing up for shifts with the data you need and which direction it flows. And it shifts again depending on which Epic site you’re connecting to.
Epic is the dominant acute-care EHR in US hospitals, so for a lot of health-tech teams, Epic EHR integration decides whether the product is adoptable across those institutions at all. Get it right and you’re inside the clinician’s workflow. Get it wrong and you’ve built a demo no one can deploy.
This guide is the working version of that: what Epic’s USCDI on FHIR APIs hand you for free, where the write-back wall sits, what site-by-site approval costs in time and budget, and what changes once the app lives on a phone. That free read-only access exists because federal interoperability regulations made standardized FHIR APIs a certification requirement for every EHR. If you’re about to develop a healthcare app on top of Epic, this is the terrain.
Key takeaways:
- Epic’s USCDI on FHIR APIs give you free, read-only access to a standard set of patient data (labs, medications, problems, vitals, demographics) across the hospitals running Epic, enough to power a clinician-facing app, a telehealth view, or analytics without paying per call.
- You can’t write back through the open APIs. You can pull data out, but you can’t place orders or push anything back into Epic. Build for reading and displaying, and keep clinical decisions inside Epic where they belong.
- Security is what gets apps rejected. Features come second. OAuth 2.0 with PKCE, least-privilege scopes, and per-site registration are table stakes, and every Epic customer approves your app on their own timeline. Build the per-site approval window into your schedule from the start.
Table of contents:
- What Epic integration actually means
- Benefits of Epic EMR/EHR integration
- Common use cases for Epic integration
- Challenges and limitations of Epic API integration
- How to integrate with Epic EHR
- 2026 considerations when integrating your mobile app with Epic EHR
- Epic integration timeline and cost
- Why health tech teams choose Topflight for Epic integration
- Let’s build a health app integrated with Epic EHR
What Epic integration actually means
“Epic” gets thrown around as if it names one system you plug into. It doesn’t. Epic is a family of slightly different deployments, and “integration” can mean reading a patient’s labs, launching your app from inside a clinician’s chart, or exporting a whole cohort for analytics. The work and the cost change with each.
What is the Epic USCDI API?
USCDI stands for United States Core Data for Interoperability. It’s the federal standard that says which classes of health data an EHR has to expose through APIs so other apps can read them. ONC maintains it, and it’s the baseline for nationwide health data sharing.
The Epic USCDI API is that standard turned into endpoints: the rules for pulling USCDI-formatted health records out of Epic.
FHIR (Fast Healthcare Interoperability Resources) is the format those records travel in. It’s a REST API plus a spec for how each piece of clinical data should be structured, so a lab result looks the same coming out of Epic as it does coming out of any other FHIR server. That consistency is the point of Epic interoperability: your app parses one shape and handles every FHIR server the same way.
![]()
What you get for free matters here. USCDI v3 is available to developers at no cost on open.epic, alongside 750+ no-cost APIs and interfaces, and Epic is building FHIR APIs for the newer USCDI v5 data set on top of that. v3 has also been the federal floor since January 2026, so it’s the version you can count on being live almost everywhere.
And the reason any of this is worth your time: Epic is where the patients are. In KLAS’s 2025 market-share report, Epic ran 43.7% of US acute-care hospitals and 56.9% of beds. If your customers are hospitals, most of them are on Epic.
Epic integration is really four different builds
What you build when you integrate with Epic depends on the data you need and which direction it moves. A few distinct paths sit under the same “Epic integration” umbrella:
- Read clinical data via USCDI on FHIR. Pull labs, meds, problems, vitals, and demographics into your app. Free and read-only, the usual starting point.
- Launch from inside Epic via SMART on FHIR. Your app opens in the clinician’s chart with patient context already passed in, so it feels like part of Hyperspace instead of a separate tab.
- Export populations via Bulk FHIR (Flat FHIR). For cohort reporting or payer programs, pull group-level datasets in one request instead of thousands of single-patient calls.
- Move legacy messages via HL7 v2. For ADT feeds and order/result flows that predate FHIR, you’re often still on HL7 v2 interfaces, sometimes routed through an engine like Mirth.
These aren’t interchangeable. A read-only telehealth view and a population-analytics pipeline are different builds with different approval paths, even though both count as integrating with Epic EHR. Scope the path before you scope the timeline.
Every Epic site is configured a little differently
Here’s the part that catches teams treating Epic as one endpoint. Every Epic customer site is configured differently, so the same app can behave differently from one hospital to the next.
The FHIR version isn’t uniform. Some sites still expose DSTU2 or STU3 resources while newer ones run R4, and R4 is what you should build against where you can. USCDI support lags too: a site might still be on v3 while the standard has moved ahead, because Epic ships newer versions release by release and each hospital upgrades on its own schedule. Then there’s approval. Every Epic customer authorizes your app against their own instance, on their own timeline, regardless of any certification you already hold. And the sandbox you tested in won’t match production exactly, since filters, available resources, and scopes shift between the two.
None of this blocks you. It just means “we integrated with Epic” really means “we integrated with this Epic site,” and the next hospital is a fresh configuration cycle. That site-by-site reality turns Epic systems integration into an ongoing program, so plan for the multiplier from day one.
Benefits of Epic EMR/EHR integration
Connecting your app to Epic does two things at once: it gets you the patient data you need, and it makes your product deployable in the hospitals that run Epic. The benefits of Epic integration mostly trace back to those two.
Start with the economics. Epic’s USCDI on FHIR gives you free, one-way patient data sync from Epic into your app, plus free access to the specs. You read it, run AI on it, whatever your product does with clinical data, without paying per call. This is the cheapest entry point into Epic EMR integration, and for a lot of products it’s enough on its own. It also replaces manual chart pulls or pricier options like HL7 v2.x feeds and CCDs (continuity of care documents). When a FHIR read covers the use case, it’s the cheaper path and the easier one to grow site to site.
Also Read: Why FHIR is no longer optional
1. Reduce data silos across healthcare departments
When radiology, lab, and pharmacy all read from the same Epic record, your app stops being one more login. Pull from Epic as the source of truth and a clinician sees current data in your tool without bouncing between systems. That’s the foundation for better care coordination: everyone works from the same chart, so patient care coordination doesn’t hinge on someone manually reconciling three screens.
2. Improve clinical outcomes with better data continuity
Structured, current records are what make downstream clinical decision-making any good. Feed an app real labs and problem lists instead of stale snapshots and your risk scoring or treatment-plan logic has something real to work with. That data continuity is the difference between a model that nudges patient outcomes and one that’s guessing.
3. Minimize manual entry and improve data exchange
Every field a clinician re-keys is a chance to introduce an error and a reason to dislike your app. Reading structured data straight from Epic over FHIR removes whole categories of manual entry, along with the one-off middleware that usually comes with it. Standard endpoints also mean less to maintain when a site upgrades.
Done right, this is where you optimize workflows that used to eat clinician time:
- chart updates that populate from Epic instead of by hand
- medication and allergy lists that arrive structured
- demographics that don’t get typed twice
4. Enable interoperability and workflow automation
Build on Epic’s FHIR APIs and you’re building on the same standards every other modern EHR is adopting, so the work travels. That’s what turns a one-off connector into scalable solutions you can extend to Cerner or athenahealth later instead of starting over. It’s also why Epic integration with other information systems tends to get easier after the first one, and why the strongest Epic integration solutions are designed for reuse from the start. The patterns repeat.
Beyond Epic interoperability, integration is what makes EHR process automation possible. With CDS Hooks you can surface alerts and recommendations at the point of care instead of making clinicians dig for them. And once Epic is the source of truth, the repetitive clinic management work automates:
- appointment scheduling
- medication reconciliation
- chart updates
- intake and check-in
That’s the core of Epic automation, and it’s where clinicians actually feel the integration.
One caveat to set expectations on: Epic’s open APIs don’t do continuous, live two-way sync. You architect around scheduled or event-driven updates, which works for most use cases as long as you plan for it up front.
5. Improve patient engagement via Epic MyChart
MyChart is Epic’s patient portal, and it’s also the easiest on-ramp for patient-facing features. Tie your app into MyChart and patients get one place to:
- view test results
- request prescription renewals
- schedule appointments
- message their care team
Lower the friction on those and patients stay engaged with their care between visits, which is increasingly where healthcare delivery happens. You get better adherence and fewer no-shows, without standing up your own portal and auth.
Common use cases for Epic integration
The free USCDI on FHIR read path covers a specific shape of product: provider-facing apps that need to read standard patient data and never write anything back. An integration with Epic built just to read is the cheapest, fastest way in.
A read-only integration with Epic EHR is the right call when:
- you’re building a provider-facing app that pulls fairly standard data: medications, allergies, conditions, demographics, test results, the contents of the Epic electronic medical records
- you want that data cheaply and want it to grow across sites without per-call fees
- you don’t need to launch your app from inside Epic
- you don’t need to push data back into Epic
Done well, that kind of Epic software integration quietly improves practice management: patient care coordination flows between systems instead of living in someone’s head, and the same pattern carries from a single clinic to a multi-site group. For smaller operations, this is often the backbone of clinic management.
Two builds where it lands cleanly. One is a telehealth app that pulls a patient’s record in mid-visit, so a remote provider sees current meds, problems, and recent labs without the patient reciting their history. Read our telehealth EHR integration guide for the deeper version.
The other is a patient management app with a simple interface that tracks treatment plans over time. It pulls the initial clinical picture (medication status, test results) when a record is first reviewed, then keeps watching for changes.
Here’s a screenshot from an MVP we built to show how little it takes to stand up a simple Epic-connected app on USCDI on FHIR.
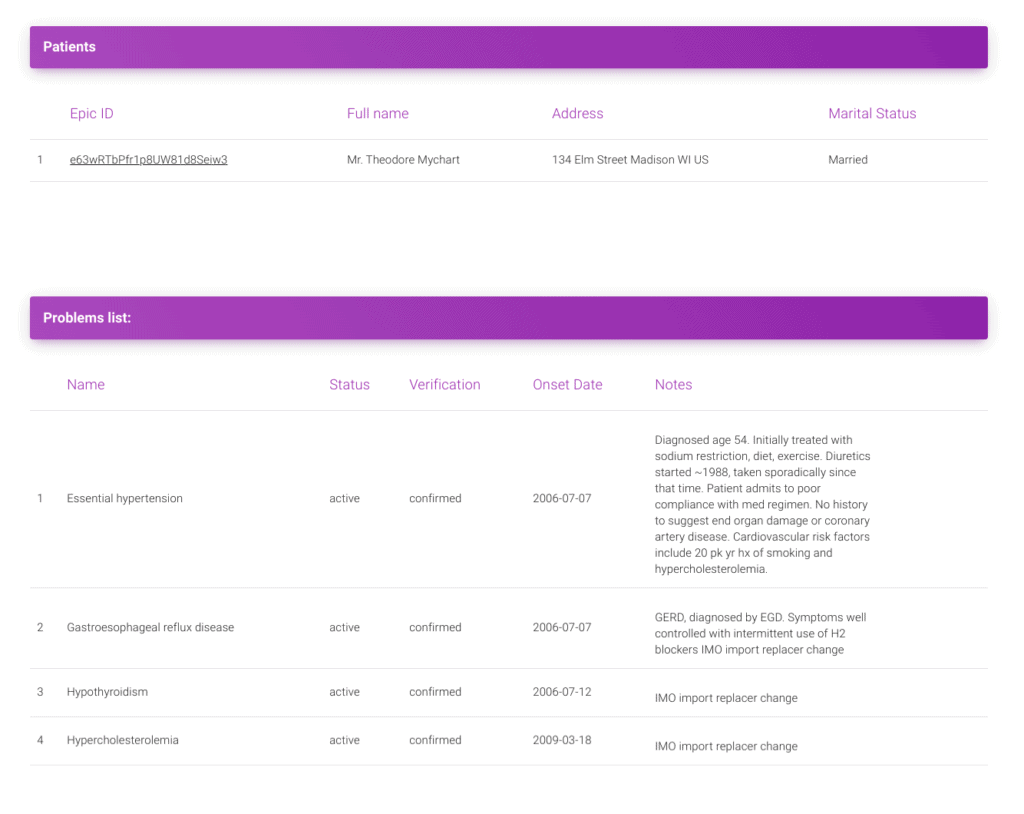
You search for a patient, then view her record: previous diagnoses, prescribed medications, care plans, plus demographics pulled in through the integration. That’s useful for a remote encounter or any downstream processing.
These read-only patterns are the Epic integration solutions most teams ship first. The more involved Epic integrations (SMART launch, write-back, bulk export) come later. If you want yours scoped against your actual product, see our EHR integration services.
Challenges and limitations of Epic API integration
Epic’s open APIs are generous for reading and stingy for almost everything else. Most of the friction of integrating with Epic is predictable. It clusters around write-back limits, per-customer governance and auth, and the reality that no two Epic sites behave the same. Know the boundaries up front and you design around them. Find them in production and you eat the rework.
Site-specific approvals and governance
There’s no single “connect to Epic” switch. Every Epic customer authorizes your app against their own instance and signs off on their own timeline, no matter how many sites you’ve already cleared or what certifications you hold. Governance lives with the customer, so the same app can clear fast at one site and stall at another. Larger health systems route it through their own IT governance, and approvals vary across institutions even inside one network. Plan for a per-customer approval cycle. Every site is its own gate.
Patient-facing apps add a wrinkle. Patients authenticate with the credentials from their MyChart-linked Epic portal, and not every facility offers one. Even where they do, you’re asking patients to remember and use those credentials, which is its own adoption tax. And on the free tier, only a subset of data is exposed to patients, so confirm what’s actually available before you promise a feature.
You can build and submit a patient-facing app on Epic’s FHIR APIs, but approval timelines swing widely with app type and each Community Member’s security review. Don’t put a fixed turnaround on the roadmap.
Related: Building a doctor on demand application
Authentication, scopes, and app registration
Most early auth pain shows up as 401s and 403s, and it’s almost always a scope or audience mismatch: the SMART scopes your app requests don’t line up with what you registered in Epic’s Connection Hub. Decide up front whether you need user-level or system-level scopes, since they’re approved and behave differently, and keep your consent screens and audit trails documented from day one. Reviewers ask for them.
Two rules from Epic aren’t negotiable. Credentials and tokens never leave Epic’s flows and are unique per Community Member, so don’t share a token across sites or hand it to a non-Epic backend. And direct database access is off the table, always. Everything goes through the official FHIR, HL7, or Epic-supported APIs, with no backdoor queries.
Data availability, workflow limits, and version drift
The Epic EMR integration API is built for reading. Through FHIR you can pull demographics, problems, lab results, medications, clinical notes, and vital signs, then build whatever sits on top, like population health dashboards and risk scoring. That’s the 80% case, and it’s well supported.
The ceiling is write-back. You can do some indirect data entry, like creating draft orders for a provider to review or filing clinical notes and observations, but final order placement stays inside Epic by design. A deeper integration with Epic EMR that needs to push real orders or live two-way sync takes more than the open APIs. Here’s what those APIs won’t do:
- place orders directly (labs, meds); CDS Hooks can hack around it, but it’s clunky and not for production
- continuous, real-time bidirectional sync; you get near-real-time or periodic, so architect for async and event-driven updates
- override Epic’s native workflows like medication reconciliation or problem-list management
- deeply customize Epic’s UI; you can launch your app via SMART, but the chrome stays Epic’s
For analytics, don’t extract huge volumes through single-patient calls. Use Bulk FHIR (Flat FHIR) to export group-level datasets in one pass, where the site’s Epic version supports it (generally August 2021 and later).
When integrating with Epic, treat version drift as a given. Some sites expose DSTU2 or STU3 resources while others run R4, and USCDI support lags release to release. Ship an adapter layer that normalizes resources across versions and gate features by what each site actually supports. A per-site conformance checklist with contract tests catches the rest.
Patient matching is the other quiet trap. MRN-only matching produces duplicates and false matches, so run an EMPI strategy that blends deterministic and probabilistic matching and keep an eye on the false-match rate.
And across infrastructure that old, billing and specialized coordination sometimes still need their own interfaces alongside the FHIR read.
Rate limits, testing, and production readiness
The gap between “works in the sandbox” and “works at the customer’s site” is where timelines slip. A few things to engineer for before you call it done:
- Rate limits and pagination. Expect 429s, and implement exponential back-off plus incremental sync (using since/lastUpdated) so a big history pull doesn’t hammer the endpoint or block your UI.
- Sandbox is not production. Filters and available resources differ between the two, sometimes with extra extensions in play. Keep per-site configs behind feature flags and validate against the actual Community Member sandbox you’ll launch with.
- Data hygiene at ingest. Normalize timestamps to UTC (ISO 8601) and clinical units to UCUM. Reject ambiguous values at the door rather than downstream.
- Per-site go-live. Each customer is its own production cutover, so a “done” integration is really done once, then repeated per site.
None of this is exotic, but it’s the work that separates a demo from something a hospital will run in production, where every interaction with the live system has to be predictable and logged. Getting an experienced team in early is usually cheaper than discovering these in a go-live week.
Also Read: Developing a Senior Care Application
Best practices for working within Epic limitations
None of the limits above are dealbreakers if you build with them in mind. Five habits that keep an Epic integration out of trouble:
1. Complement Epic’s native functionality
Build your app to sit alongside the core EHR rather than reinvent it. Providers want a clean handoff between your tool and Epic. Make them bounce between conflicting screens and they’ll quietly stop using you.
2. Plan for asynchronous data flows
Since live two-way sync isn’t available, design for async from the start. Lean on Epic’s notifications and webhooks so your app refreshes when something actually changes.
3. Stick to open standards
Stay on FHIR and HL7 wherever you can. Standard data exchange keeps you compatible across sites and makes the jump to another EHR far less painful later.
4. Engage Epic and your IT team early
Sort out permissions and constraints before anyone writes code. The teams that loop in Epic support and the customer’s IT and clinical owners early hit far fewer surprises mid-build.
5. Focus on data presentation over direct write-back
Most of the value you can deliver doesn’t require writing anything back. Surface the clinical summaries and risk scores that sharpen decision-making, and let Epic stay the system of record. That single choice sidesteps a huge share of the approval and compliance friction.
Stick to these and your app fits into Epic’s world while standing on its own merits, with less clinician friction and a build that stays inside Epic’s compliance lines.
How to integrate with Epic EHR
Before anything else, confirm the sites you want to pull from are on a supported Epic version. Most are, but the account or integration manager at each site can verify it. After that, how to integrate with Epic EHR comes down to a short sequence: start at open.epic.com for Epic’s developer resources and onboarding, use the Epic on FHIR docs and sandboxes to validate the endpoints you need, then line up registration and enablement with the specific Epic Community Member you’re working with. The account you create at open.epic.com or fhir.epic.com is the same one you’ll use to register the Epic EHR API.
What data can you access through Epic APIs
Related: EHR/EMR Software Development: The Ultimate Guide
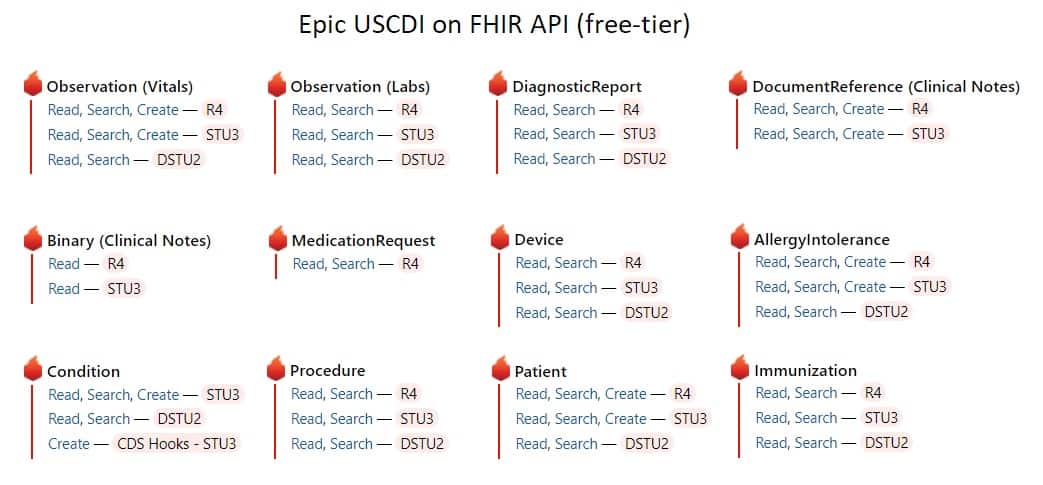
USCDI sets the floor for what’s free: the minimum dataset every certified EHR has to expose. It widens a little each year, but don’t assume you can pull anything you want. Here’s the kind of data typically available on the free tier through Epic’s FHIR APIs:
- Observation (Vitals): vital signs
- Observation (Labs): lab results
- DiagnosticReport: things like radiologist reports for imaging studies (the images themselves aren’t included)
- DocumentReference and Binary: clinical notes from clinical staff
- MedicationRequest: prescribed medications
- AllergyIntolerance: a patient’s allergies and intolerances
- Condition: problem-list entries
- Procedure: surgeries, endoscopies, biopsies, physiotherapy, and similar
- Patient: demographics and other administrative info
- Immunization: vaccines and administration details
- Device: implantable device info, the foundation for medical device ehr integration
Plenty of these USCDI-aligned APIs are no-cost through Epic’s public developer resources. But access to specific operations, including any write workflows, and production enablement can vary by API and by Community Member. Confirm what your target site actually exposes early in onboarding.
Also Read: Mastering PointClickCare EHR Integration
What you need to integrate a health app with Epic
Also Read: EHR Implementation Guide
Three pieces, at minimum:
- a server running your app, whether that’s an AI app analyzing patient data to surface a preliminary read, or a simple tool that displays readings and links to resources
- the FHIR integration itself: a REST API wrapped in OAuth 2 that authenticates the user and pulls records into your app
- your app registered with Epic
The real work is the middle one. You’re building a data exchange layer that lets your app interface with Epic’s backend cleanly and securely. To use the full set of Epic resources, you’ll want a developer account in Epic Connection Hub on Epic Showroom, Epic’s app store for health apps. From there your app can run on its own against Epic over the API, or run inside Hyperspace, Epic’s workspace for providers.
Also Read: E-Prescription App Development Guide
Epic FHIR API implementation guide
Once you know which sites you’re targeting, the build follows a repeatable shape. Scope the USCDI resources your product needs, then map each one to the FHIR version each site exposes. Build against R4 where you can, and gate the older DSTU2 and STU3 paths behind capability checks.
Define an endpoint-and-scope matrix per site so you’re not guessing what’s enabled where. Implement paging and real error handling for every interaction with Epic’s endpoints (expect 401, 403, 410, 422, 429), with back-off on the rate-limited ones. Then validate against the actual Community Member sandboxes you’ll launch with, and keep a per-site conformance checklist so a new site is a checklist run instead of a fresh investigation. That matrixing is the single biggest thing that keeps rework down as you add sites.
OAuth 2.0 authentication for Epic integration
Default to the Authorization Code flow with PKCE (Proof Key for Code Exchange). Epic has supported PKCE since August 2019 and strongly recommends it for native mobile apps, so there’s no reason to skip it. Scope to least privilege, register your client per site, store tokens in the OS keystore, and rotate refresh tokens.
For provider sign-in, use the Standalone Launch defined in Epic’s FHIR spec. It runs on standard OAuth 2.0, so you avoid building and maintaining your own credential infrastructure. On older deployments where PKCE isn’t available, fall back to Universal Links on iOS and App Links on Android for deep links, and enable offline access through dynamic client registration where it’s supported. And the rule from earlier still holds: tokens and credentials stay inside Epic’s flows, never handed to a non-Epic backend.
Epic Connection Hub on Epic Showroom certification process
A quick terminology check, because the old names cause real delays. Epic’s current marketplace is Showroom, launched in 2024. It has three tiers: Connection Hub (the basic listing for third-party integrations, around $500 a year and where most apps live), Toolbox (curated integration patterns), and Workshop (deep co-development, invite-only). App Orchard and App Market are retired. If a hospital’s IT team tells you to “get listed in App Orchard,” that program no longer exists, and clearing that up early saves weeks.
Start by creating a developer account, which runs through Epic Vendor Services, and register your app with the exact FHIR resources and scopes you’ll request in production. Match your privacy and consent copy to what users see at install. Validate in the Community Member sandbox you’ll launch with and document the per-site quirks, then complete Epic’s attestation and security checklists before requesting a Connection Hub listing. The listing review itself usually runs 8 to 16 weeks, so build it into the timeline rather than treating it as a formality at the end.
2026 considerations when integrating your mobile app with Epic EHR
Epic already ships mobile apps: MyChart for patients, Haiku and Canto for providers. So before you build, ask whether you should. For a lot of teams the answer is yes, because the stock apps don’t cover the specific workflow they need, and the app-store ratings make the gap visible.
Why build a custom mobile app on top of Epic
MyChart, Haiku, and Canto are built for the general case. They handle standard patient and provider workflows, and for plenty of organizations they’re enough. The reason to build your own is a use case they don’t serve: a condition-specific patient experience or a specialty provider workflow the defaults don’t handle.
The stock-app ratings above are part of why teams consider it. When the default experience frustrates users, a focused custom app pulling the same Epic data can be a real upgrade for the people using it every day. Most of what you’ll need is documented in Epic’s developer FHIR toolbox and its interoperability guide.
Define your mobile app’s data, workflows, and exchange direction
Three decisions up front save you from expensive rework later.
First, the data. Which resources does your app actually touch, and at what level of detail? Demographics and a medication list are a light lift. Full clinical history with attachments is a much bigger one.
Second, the direction. Are you reading from Epic, writing back, or both? On mobile that mostly means reading, given the write-back limits we covered, but be honest about it now, because it shapes everything downstream.
Third, the workflows. Pin down exactly when the data exchange happens, say at scheduling or during an encounter. The workflow is what decides which APIs you call and when.
One mobile-specific note while you’re here: treat the phone as the edge of your PHI boundary. Store on-device data in the OS keystore or secure storage, and enforce inactivity time-outs.
Choose the right data exchange method for mobile use cases
For a mobile build, the exchange method usually picks itself, but be deliberate about it. Match the method to the use case:
- reading clinical data into the app: USCDI on FHIR (R4) over REST, authenticated with OAuth 2 and PKCE, the default for almost every mobile use case
- launching from inside Epic on a provider’s device: SMART on FHIR, so your screen opens with patient context already in hand
- population or cohort work: a backend Bulk FHIR job, not something the phone should be doing
- legacy feeds (ADT, orders, results): still HL7 v2 on the backend, surfaced to the app after your server processes it
The phone talks FHIR. Anything heavier, like bulk exports or v2 message processing, belongs on your server, with the mobile client reading clean, already-reconciled data. Keep that split clear and the app stays responsive and easier to secure.
How patient-facing FHIR responses can differ across Epic environments
If you’re building anything patient-facing, expect the same FHIR call to return different data at different sites, and sometimes for different patients. Epic and its customers filter patient-facing responses for privacy and relevance, so plan for variation rather than assuming a clean, uniform payload.
What drives the differences:
- Responses are scoped to the authenticated patient, so what comes back depends on who’s logged in.
- Patient-entered or freshly filed data may not appear until a clinician reviews and reconciles it.
- Some responses use patient-friendly terminology instead of raw clinical codes.
- Certain lab results can be withheld to comply with state and local law.
- A site can turn that filtering off, in which case responses look more like the provider-facing version.
Because each customer configures this differently, Epic’s own advice is to test every API at each Community Member site before you go live. Budget for that testing per site, the same way you budget for per-site approval.
Also Read: Patient Intake Management Automation Guide
Supporting SMART Health Cards in mobile apps
If your app touches vaccine or test credentials, you’ll run into SMART Health Cards. They’re an open, interoperable standard built on HL7 FHIR and aligned with W3C Verifiable Credentials, and Epic generates them in a couple of ways. What your mobile app needs to handle:
- QR codes a patient pulls from MyChart, on screen or downloaded
- QR codes a health system generates for patients who don’t use MyChart
- QR codes shared from another device or printed on paper, so read both screen and paper reliably
- the .smart-health-card file itself, by associating your app with that extension so a download opens in your app
Get those input paths right and a patient can present a credential however they happen to have it, which is the whole point of the standard.
Related Article: SMART on FHIR Guide to Healthcare App Development
Cross-network exchange and TEFCA considerations
One shift worth planning around: TEFCA is live and moving fast. It went live in late 2023, and there are now nine designated QHINs (Qualified Health Information Networks). Epic’s own QHIN, Epic Nexus, is how Epic organizations plug into that nationwide mesh.
For cross-network use cases, like payer exchange, multi-system cohorts, or letting a patient pull their records from any Epic site, this matters. Through Epic Nexus and Individual Access Services (IAS), an app can reach Epic data across organizations rather than integrating with Epic EHR site by site for every connection. Adoption is moving quickly: well over a thousand Epic hospitals and tens of thousands of clinics are live or onboarding, and TEFCA document volume jumped from roughly 10 million in 2024 to hundreds of millions by the end of 2025.
So track TEFCA in parallel with your direct Epic plan. For some products it’s an alternative on-ramp to the per-site integration grind, especially anything patient-facing built on IAS. We’re only scratching the surface here, so if you want this mapped against your actual Epic setup, that’s a conversation worth having.
Epic integration timeline and cost
Before the technical weeds, know what you’re committing to. Most Epic integrations run 6 to 12 months and cost $50,000 to $200,000+, depending on complexity. Here’s where the time and money go.
Time and cost by phase
The phases break down roughly like this. Times and costs scale with complexity, so treat these as planning ranges rather than firm quotes.
| Phase | Time | Cost factor |
|---|---|---|
| Application & Showroom registration | Days to 4 weeks | Minimal fees ($500–$1,900/year for Connection Hub or Vendor Services); the main cost is internal time spent identifying customer sponsors and preparing documentation |
| Sandbox development | 2–6 months | The largest investment, where developer hours dominate. Budget $50,000–$150,000+ for a small team of 2–3 engineers. Vendor Services membership ($1,700–$1,900/year) is required for proprietary API access |
| Validation & certification | 1–4 months | Security and compliance testing ($20,000–$80,000), SOC 2 or HITRUST certification ($30,000–$100,000+ if required), and legal/BAA negotiations |
| Production go-live | 2–4 weeks per site | Deployment and configuration ($5,000–$15,000/site), training (~$2,000), and go-live support ($10,000–$30,000). Note: each Epic customer must individually approve access |
What usually increases time and budget
A few things reliably push toward the high end of those ranges.
The sandbox eats the most budget. Epic’s free FHIR sandbox at fhir.epic.com is a solid start, but expect sparse docs and periodic environment resets that force you to rebuild test cases. Anything beyond standard FHIR, the proprietary APIs, needs a Vendor Services membership on top.
Validation scales with what you’re building. A read-only FHIR app can clear in weeks. A bidirectional integration that touches clinical workflows takes months of back-and-forth with Epic’s review teams, plus a separate security assessment at each health system you connect to.
Production multiplies. Every customer site needs its own approval and configuration regardless of the certifications you hold, so each new system repeats part of the validation cycle. A “done” integration is done per site.
Middleware is the main lever in the other direction. Platforms like Redox can compress development timelines by 30 to 40%, trading some control for convenience. Their annual platform costs run roughly $11,000 to $270,000 depending on volume, so it’s a real line item worth modeling against the engineering time it saves.
For a deeper look at cost drivers, see our EHR Implementation Cost Breakdown and Epic EHR pricing guides.
Why health tech teams choose Topflight for Epic integration
When timelines are tight and PHI is on the line, you want a team that’s already shipped real Epic integrations. We have. The products we’ve built have helped clients raise $188 million+ in follow-on funding, because a tight EHR integration is what makes a health-tech product adoptable in the first place.
We’ve shipped, tested, and listed apps in Epic’s Connection Hub and the Athena Marketplace, so we know the sandbox quirks and the checkboxes standing between you and clinical adoption. That’s the short version of our Epic EHR integration services. Here’s what working with us actually looks like.
Marketplace and listing experience
Getting an app into a clinician’s hands is a listing and onboarding problem as much as an engineering one. We manage the whole path from developer account to live listing, including the Connection Hub and Athena Marketplace paperwork that stalls most teams. When a listing or attestation needs to move, we’ve walked it before.
Deep Epic, FHIR, and HL7 delivery expertise
Real Epic work spans modern and legacy in the same project. Our engineers handle SMART on FHIR and R4 resources alongside the dusty HL7 v2 messages a lot of sites still run on, and they keep the data flowing without tripping an auditor. That range, FHIR and HL7 under one roof, is what a lot of Epic integration services are missing.
Compliance and security built into delivery
The compliance work ships with the build. HIPAA, OAuth 2 with PKCE, SOC 2, audit artifacts: the boring, necessary parts are handled as part of delivery, so they’re done while you focus on the product. That ordering matters in healthcare, because retrofitting compliance after the fact is where budgets quietly blow up.
Faster time to market without reinventing the process
Most of the integration playbook is already built, so we’re not starting from scratch on yours. Pre-built components and a process we’ve run many times mean you demo to clinicians while competitors are still stuck in vendor paperwork. Speed here buys something specific: time in front of clinical users early, while there’s still budget to act on what you learn.
Proven results in Epic-connected products
A couple of Epic-connected products we’ve shipped, and what came of them.
Roundr
Roundr is a cross-platform rounding app for hospitalists, built for quick EHR access and clean charting on the move. We connected it to Epic over FHIR and HL7 v2 (ADT) using Mirth. Early clinician feedback points to faster rounds and smoother note workflows.
GaleAI
GaleAI automates medical coding, and the numbers are the story: a 97% cut in coding time, up to 15% higher revenue from better coding accuracy, and 7.9% more codes than human coders in a one-month audit, which surfaced about $1.14 million in annual underbilling. It runs on SMART on FHIR with Epic and Athena integrations.
What clients say
“Topflight built our iOS/Android app and transformed an idea into a working tool.”
Dr. Josh Dégallier, Roundr
“End-to-end help getting software into users’ hands: design, testing, integrations.”
Grant Muller, MD, GaleAI
DIY vs. Topflight professional integration
If you’re weighing an in-house build against bringing us in, here’s the honest side-by-side.
| Decision area | DIY (internal team) | Topflight |
|---|---|---|
| Time-to-first connection | Weeks to months of environment setup, scope mapping, and sandbox quirks | Prebuilt playbooks; per-site conformance matrix; faster path to demo |
| FHIR version drift (DSTU2/STU3/R4) | One-off patches; risk of regressions | Adapter layer plus feature gating per site; regression tests baked in |
| OAuth 2.0 (PKCE, consent, DCR) | Security reviews slow releases | PKCE and least-privilege scopes implemented routinely; audit artifacts ready |
| Marketplace listing (Connection Hub) | Paperwork ping-pong; unclear checklists | Guided onboarding and review prep; partners for certified needs when required |
| Sandbox vs. prod deltas | Surprise filters, extensions, and scope errors late | Site-by-site configs; contract tests; staged rollouts |
| Identity & EMPI | MRN-only risks duplicates and false matches | EMPI strategy (deterministic plus probabilistic) with monitoring |
| Cost risk | Overruns from rework and delays | Fixed-scope milestones; reuse of proven patterns from past Epic work |
When certification or listing is in scope, we coordinate with Epic Connection Hub and Showroom certified partners and manage the submission and QA steps while keeping your build moving.
Let’s build a health app integrated with Epic EHR
Epic gives you a lot to work with, even though official support stops at the posted docs. That’s where we come in. We help teams get past the roadblocks the documentation doesn’t cover, including the data questions and medical device integration edge cases, and there’s an active Google Group that fills some gaps around the Epic USCDI API.
If you’re scoping an Epic EMR integration or Epic EHR integration project, the details are where things go sideways: the patient search feature, the parameters in your patient search API calls, the quirks in whatever API documentation you’re working from. Working with people who’ve shipped Epic integrations before means your app supports Epic systems integration cleanly and keeps patient care coordination intact across institutions.
Tell us about your Epic setup and what you’re trying to build, and we’ll map the path.
Other blogs about healthcare app development:
- How to build a healthcare chatbot
- Guide to creating a Hospital Management Software
- Blockchain in Healthcare: The Good, Better, Best
- A Guide to Integrating AI in EHR
Related articles:
- Healthcare App Development: Everything you need to know
- Healthcare Mobile App Design Guide
- How to Start a Healthcare Startup
- A Guide to Medical Website Development
- HIPAA Compliant App Development Guide
- Cost of EHR Integration
- Cerner vs EPIC: The Better Choice?
- Seamless Data Migration for EHR
- Cost of EHR Implementation
[This blog was originally published in May 2020 and has been updated since.]
Frequently Asked Questions
What is the Epic USCDI API?
It’s the set of FHIR rules for reading USCDI-formatted health data out of Epic. USCDI is the federal standard that defines which classes of health data a certified EHR has to expose, so the API gives you a predictable way to pull that data into your app.
What is Epic integration?
Connecting a third-party app to Epic’s EHR to exchange patient data securely, usually through FHIR-based APIs. Depending on the use case it can mean reading clinical data, launching your app inside Epic, or exporting populations in bulk.
How does Epic integration improve healthcare workflows?
By syncing clinical data between your app and Epic in near real time, it cuts redundant data entry and keeps clinicians working from one current record instead of several screens. That tightens coordination across departments.
What factors influence the cost of Epic integration?
Scope is the big one: read-only versus bidirectional, paid versus free APIs, workflow complexity, middleware, and whether you need a Connection Hub listing. Most projects land between $50,000 and $200,000+ over 6 to 12 months.
What is FHIR?
Fast Healthcare Interoperability Resources. It’s both a REST API for exchanging health records and a spec for how that data should be formatted, so the same clinical data looks consistent across any app that supports it.
How can I benefit from using Epic USCDI on FHIR?
You can build medical software that pulls patient data from Epic at no cost. Epic offers USCDI v3 support free to developers on open.epic, alongside hundreds of other no-cost APIs and interfaces.
Can I sync any patient-generated data (say, from a medical sensor) back to Epic?
Not through the open USCDI API. It’s read-only, so you can load data from Epic into your provider-facing app, but pushing patient-generated data back into Epic takes different APIs and approvals.