
Your attorney just told you you’re a business associate. Or a health system’s security review confirmed it: you handle protected health information, so HIPAA applies to you directly, as a covered entity or business associate. The clock’s running, and year one HIPAA compliance is suddenly your problem. This is the playbook for that first year: the order to do it in, and what each phase costs.
Keep one distinction in mind. What HIPAA requires, what a defensible security program needs, and what an enterprise buyer makes you buy are three different things. SOC 2 and HITRUST live in that third bucket. HIPAA itself doesn’t require them, so don’t let anyone tell you that you need them to comply.
We’re assuming you’ve settled whether HIPAA applies. If you haven’t, the scope check below sorts it out: for building from scratch, start with HIPAA compliant app development; for AI tools, see HIPAA compliance AI-generated code. The HIPAA Year 1 roadmap here picks up where those leave off.
OCR closed 21 settlements in 2025, its second-highest total on record, and its Risk Analysis Initiative hit 13 by April 2026, widening into risk management. Talk to your attorney. Then get to work.
What does year 1 HIPAA compliance actually take for a digital health startup?
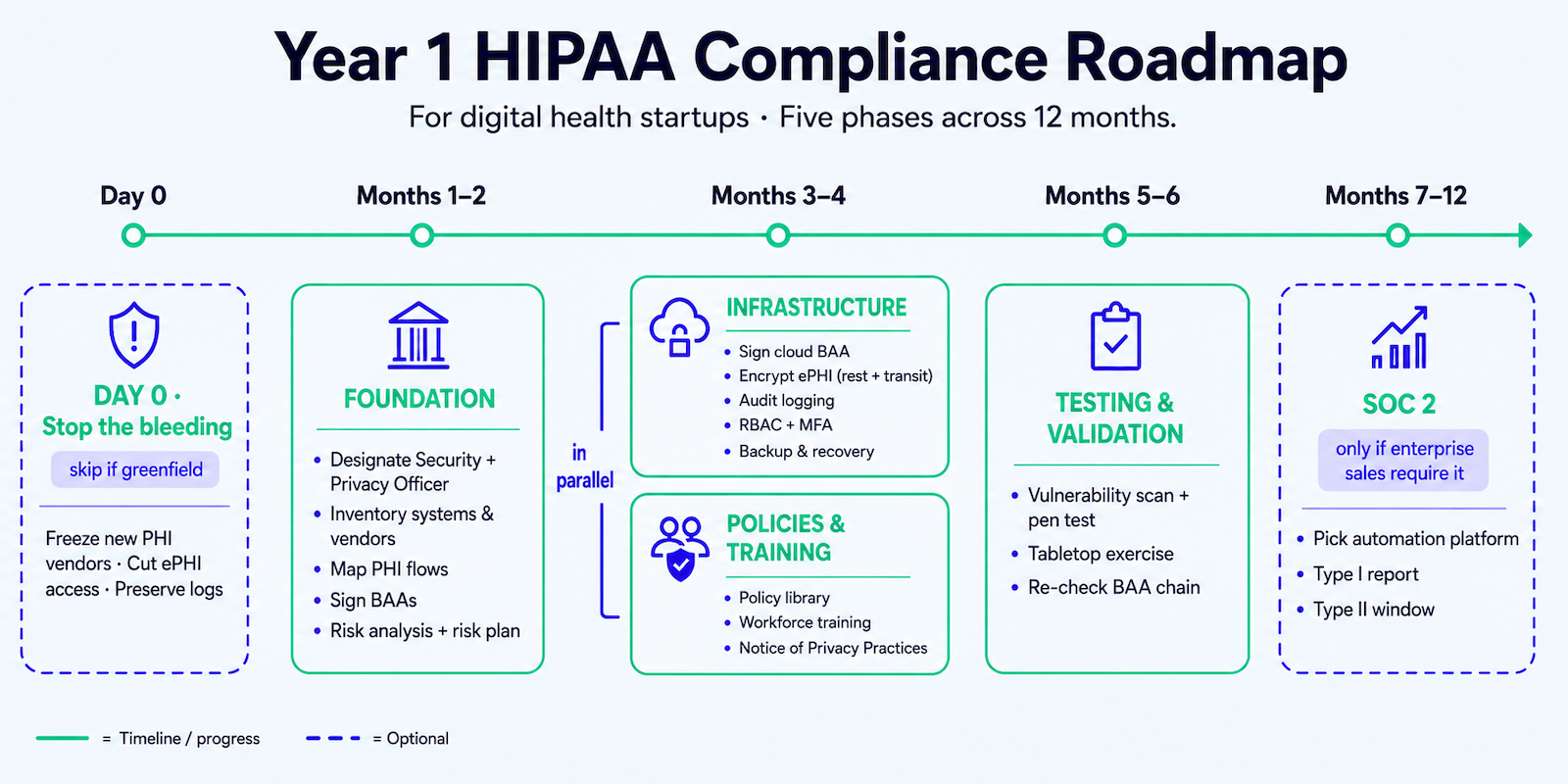
Work it as five phases across 12 months: inventory your systems and map every PHI flow, run a risk analysis scoped to that map, close every BAA gap before PHI starts flowing, build infrastructure (encryption, audit logging, RBAC, MFA) and policies in parallel, then test with a scan and a tabletop. Add SOC 2 only if enterprise buyers require it. The sequence is what makes it real: you can’t credibly assess risk in systems you haven’t mapped, and you can’t close BAA gaps you never found.
Key Takeaways
- Year 1 compliance is infrastructure your whole business runs on. It sits under every enterprise contract, every investor diligence pass, and every OCR interaction that follows. Build it like the foundation it is.
- Real compliance is documented evidence of controls that run. A template policy library and a green dashboard don’t survive an audit; OCR’s 2026 posture targets documentation with no implementation behind it.
- The sequence is the strategy. Map your PHI flows, scope the risk analysis to that map, close BAA gaps before any PHI flows, then add policy and training. You can’t assess risk in systems you haven’t mapped, and that order puts your foundation in by month 6, ready for any enterprise security questionnaire by month 12.
Table of Contents
- Are you actually under HIPAA? A 30-second scope check
- The Year 1 HIPAA compliance checklist, sequenced by phase
- What Year 1 HIPAA compliance actually costs
- Five gaps that survive a green compliance dashboard
- Why Topflight Apps for HIPAA-compliant development
Are you actually under HIPAA? A 30-second scope check
One of three conditions puts you under HIPAA. Run the test, then move on.
- You’re a covered entity: a healthcare provider, health plan, or clearinghouse.
- You’re a business associate: you create, receive, maintain, or transmit PHI on behalf of a covered entity (45 CFR 160.103). Most digital health startups land here.
- You’re a subcontractor of a business associate: you handle PHI for someone who’s already a BA.
If none of these fit, HIPAA doesn’t bind you directly, though state privacy law still might.
The reverse caveat matters too: some products carry more than HIPAA. Building an FDA-ready companion app usually means layering device classification and IEC 62304 work on top of everything in this roadmap.
Here’s the part founders underestimate. A business associate carries direct liability. OCR, the HHS Office for Civil Rights, can investigate and fine you, the BA, regardless of what the BAA with your covered entity says. The HITECH Act made the Security Rule’s safeguards, policies, and documentation apply to BAs directly in 2009, and the 2013 Omnibus Rule gave it teeth.
That’s what HIPAA business associate compliance actually means: you own the controls yourself, in writing. Take ambient AI scribe app development: a scribe transcribing visits for a hospital creates and transmits PHI on the hospital’s behalf, which makes its maker a business associate.
The Year 1 HIPAA compliance checklist, sequenced by phase
Map before you buy tools or write policies. Out of order is how teams burn months: you buy infrastructure you later reconfigure, write policies for systems you never inventoried, and run a risk analysis that comes back meaningless.
Here’s the HIPAA compliance checklist for startups, sequenced into phases, with the HIPAA compliance steps in the order they work. (Earlier than this, still scoping the product? Our healthcare app development guide covers that groundwork.) Phases run roughly in sequence, but infrastructure and policy work overlap in months 3–4, and SOC 2 prep starts once your controls are live.
Day 0: stop making the exposure worse (skip if you’re greenfield). Already running PHI in production? Stop the bleeding before anything formal starts: freeze onboarding of any new vendor that would touch PHI, find the analytics and telemetry tools already touching it without a BAA, cut ePHI access to who needs it, preserve your logs, and hand every known gap to a named owner.
Months 1–2: foundation
Sequence matters most here; each task feeds the next.
- Designate a HIPAA Security Officer and a HIPAA Privacy Officer. Often one person early on; HIPAA allows it, but put the designation in writing.
- Inventory every system, vendor, data store, and access point.
- Map every PHI and ePHI flow across that inventory: each system, API, vendor, and data store that creates, receives, maintains, or transmits it. A clinical medication adherence platform, for instance, routes pharmacy and claims data through several vendors before your database sees it, and each hop is a flow to map. This is PHI flow mapping.
- From that map, find the missing BAAs and unsafe flows, then sign a BAA with every vendor that touches PHI before any PHI flows: cloud host, analytics, email, support tooling, LLM APIs. (Calling OpenAI’s models on PHI has its own rules; see Is OpenAI HIPAA compliant?)
- Run the risk analysis, scoped to what you mapped. It’s the security-management standard at 45 CFR 164.308. NIST SP 800-30 is the methodology the field uses; HIPAA requires the analysis without dictating the method, and the free HHS Security Risk Assessment Tool covers smaller teams.
- Turn the findings into a risk management plan: every risk gets an owner and a date.
Done means you have: officer designation in writing, a system and vendor inventory, a PHI flow diagram, an executed BAA register, a risk analysis with a prioritized risk register, and a risk management plan with owners and dates.
Months 3–4: infrastructure
This overlaps the policy phase below; one engineer builds controls while someone else drafts policies.
- Confirm your hosting is HIPAA-eligible, then sign the cloud BAA. All three major clouds offer one: the AWS HIPAA BAA, the Google Cloud HIPAA BAA, and the Azure HIPAA BAA. A HIPAA-compliant cloud starts with that signature and the eligible service tiers.
- Encrypt all ePHI, at rest and in transit.
- Turn on audit logging for every system that touches ePHI.
- Lock down access controls: role-based access control (RBAC) and multi-factor authentication (MFA) across those systems, plus session-management timeouts so an unlocked laptop isn’t an open door.
- Stand up data backup and recovery, with RTO and RPO documented and a restore you’ve actually run.
Encryption and MFA are technically “addressable” today. Teams read that as optional and get burned: OCR has penalized teams that skipped them, and the pending update would make them required outright (more below). Build them now.
Done means you have: a signed cloud BAA, encryption at rest and in transit, audit logging on every ePHI system, RBAC and MFA enforced, and a backup you’ve restored at least once.
Months 3–4: policies and training
Run this alongside the infrastructure build.
The Security Rule (45 CFR 164.316) requires documented policies and procedures across the administrative, physical, and technical safeguards, kept six years. It doesn’t name the documents, which is where teams go wrong: a downloaded template pack reads fine until an auditor asks how it maps to your systems, and it can’t. Derive the set from your risk analysis and how you operate:
- access management and authentication
- device and media controls, including disposal
- transmission security
- incident response and breach notification
- contingency and backup
- workforce training and sanctions
- vendor and BAA management
Then complete HIPAA workforce training for everyone who can touch PHI, recording who trained and when, down to the policy version. Covered entities also publish a Notice of Privacy Practices (Privacy Rule, 45 CFR 164.520); business associates don’t.
Done means you have: a policy library tied to your risk analysis, dated training records by name and version, and, for covered entities, a published Notice of Privacy Practices.
Months 5–6: testing and validation
Controls you haven’t tested are controls you’re guessing about.
- Run a vulnerability scan and a penetration test against ePHI systems. HIPAA doesn’t mandate a standalone pen test today, but SOC 2 requires one and the coming rule proposes annual testing, so teams headed for enterprise sales do it now. (Pricing sits in the cost section.)
- Run a tabletop incident-response exercise: walk a hypothetical breach end to end, detection through notification, and see where the plan stalls.
- Re-check the full BAA chain, subprocessors included. The analytics SDK, the crash-reporting tool, and the AI API your vendor quietly calls are all in scope, and where coverage gaps hide.
Done means you have: scan and pen-test reports with remediation tracked to closure, a tabletop write-up with its fixes, and a BAA chain that reaches every subprocessor.
Months 7–12: SOC 2, if enterprise sales require it
The three-standard line in practice. SOC 2 is a buyer requirement: most health systems and pharma buyers want SOC 2 Type II on top of HIPAA before they sign. HIPAA itself doesn’t ask for it. If a deal like that is in your pipeline, start by month 6.
Pick a compliance automation platform for evidence collection and monitoring: Vanta, Drata, and Secureframe are the usual three, all gated behind a sales call. They automate maybe 80% of the grind, the evidence-gathering and monitoring. The other 20% is human work no tool does: the policy design and control implementation that hold up, plus fixing whatever the auditor flags. The platform speeds audit readiness; it can’t hand it to you.
Target a SOC 2 Type I report by month 9 or 10, then open the SOC 2 Type II observation window, typically 3 to 6 months.
Done means you have: a platform with evidence flowing, a Type I report or one on the calendar, and a defined Type II window.
On the horizon: the pending HIPAA Security Rule update
HHS published a Security Rule NPRM on January 6, 2025, the first major overhaul in over two decades; comments closed that March. As of June 2026 it’s still just a proposal. OCR pulled in 4,700-plus comments, is still working through them, and Director Stannard wouldn’t commit at HIMSS in March 2026 to finalizing it. The spring 2026 target passed with nothing published. It could land as written, land modified, slip, get republished, or be withdrawn (if finalized as proposed, you’d have roughly a 240-day window).
What it would change is concrete:
- the “addressable versus required” distinction disappears; every implementation spec becomes required
- encryption and MFA become mandatory
- vulnerability scans move to every six months, penetration testing to annual
- a 72-hour breach-notification requirement is added
- network segmentation and a maintained asset inventory become required
- business-associate oversight tightens to annual verification backed by evidence, where a signed attestation suffices today
More than 100 hospital systems and provider groups (Cleveland Clinic, Yale New Haven, Advocate, the AMA, the AAP) signed a CHIME-led letter in February 2025 asking HHS to pull it, citing HHS’s own first-year cost estimate near $9 billion. Build encryption and MFA now regardless; don’t architect as if the 2026 HIPAA Security Rule update were already law.
What Year 1 HIPAA compliance actually costs
So what does HIPAA compliance cost? Direct answer: a lean greenfield build runs $15K to $40K, an existing product with real gaps runs $60K to $120K, and enterprise-grade (SOC 2 Type II plus HITRUST) runs $150K to $300K and up.

The HIPAA compliance cost for a digital health startup splits along the three-standard line: part is the HIPAA program baseline, what compliance actually requires, and part is buyer-driven assurance, what SOC 2, HITRUST, advisory, and a security hire add once a contract demands them. And cash is only half the bill; your team’s time is the other half. What HIPAA compliant software development really costs comes down to which bucket you land in.
| Tier | Year-1 range | What drives it |
| Lean startup (greenfield, internal compliance officer, automation tool, no SOC 2 yet) | $15K–$40K | Compliance automation platform $7.5K–$25K/yr (Vanta, Drata, or Secureframe; Vanta around $10K), small-scope pen test $3K–$8K, risk analysis $2K–$5K with a tool, training. Nearly all HIPAA-baseline. |
| Mid-stage (existing product with gaps, consultant-led risk analysis, SOC 2 Type I by year-end) | $60K–$120K | Consultant fees $15K–$40K, gap remediation $25K–$50K (baseline), SOC 2 Type I audit $5K–$20K (buyer-assurance), platform license. |
| Enterprise-grade (SOC 2 Type II, HITRUST target, dedicated or fractional security lead) | $150K–$300K+ | Dedicated hire or fractional CISO $80K–$150K, HITRUST assessment $50K–$100K, SOC 2 Type II audit $30K–$75K. Mostly buyer-assurance. |
One line item that hides: platform onboarding is usually billed separately from the license (Drata lists $10K–$25K; budget $5K–$15K without an internal specialist), and the audit fee is never bundled in.
The HIPAA baseline vs what buyers make you buy
Two layers, and the gap between them is where startups overspend. The HIPAA baseline is what the regulation itself needs:
- risk analysis and policies
- workforce training
- technical controls: encryption, MFA, audit logging, RBAC
- vendor review and BAAs
- testing and remediation
Buyer-assurance only appears when a contract asks: SOC 2 Type I or II, HITRUST, outside advisory, and a dedicated or fractional security lead. A seed-stage team with no enterprise deals signed often needs only the baseline, which lands it at the bottom of that table. The Enterprise tier is mostly assurance-layer spend, almost none of it HIPAA itself. Before you write a check for SOC 2, confirm a buyer is actually asking.
Founder and engineering time is the hidden half of the bill
The dollar ranges above are only the cash side. The other line item never hits an invoice: your team’s hours. The founder or CTO runs the risk analysis and chases BAAs. Engineers implement encryption, logging, and RBAC, then fix whatever the scan turns up. Someone owns evidence-gathering and sits through the audit. SOC 2 readiness alone runs 150 to 300 hours of manual evidence work, hours a team either eats itself or pays a platform and consultant to absorb. That’s the tradeoff: buy the tools and spend cash to save time; do it in-house and spend time to save cash.
Gap remediation is the swing variable
This is the line that decides which tier you’re in. Greenfield on HIPAA-eligible infrastructure from day one and remediation is minor; a gap analysis turns up little because there’s little to fix. Inherit a product on non-HIPAA infrastructure, logging PHI into unprotected analytics, or wired to vendors without BAAs, and remediation can dwarf every other number here, because re-platforming and refactoring are the expensive kind of work. We’ve watched the same gap surface in enterprise due diligence again and again: cheap to fix before a sales cycle, brutal once a buyer’s security team has flagged it. Find out which situation you’re in before you set a budget.
Build vs. buy, capability by capability
Where to spend, and where to do it yourself:
- Risk analysis: buy the platform; don’t hand-roll the documentation. It’s the gap auditors hit hardest.
- Policy library: buy an auditor-approved baseline, then customize it to how you operate.
- HIPAA-eligible hosting: DIY on AWS, Google Cloud, or Azure if you’ve got the DevOps capacity. If not, an Aptible-style HIPAA-as-a-Service handles the infrastructure, though it’s consumption-priced and infrastructure-only, so you still layer a Vanta or Drata program on top.
- Pen testing: always buy it. (SOC 2 requires it and the new rule proposes it; HIPAA on its own doesn’t, today.)
- SOC 2 audit: buy a CPA firm and use a compliance automation platform to cut prep 50% to 75%. Platform-partner auditors beat the Big Four on price.
- BAA tracking: use the platform’s vendor module; manual spreadsheets are where BAA gaps hide.
Not sure which bucket you’re in? That’s the point of a real audit before you spend on remediation. Topflight’s Vibe to Traction System opens with exactly that: a 2-to-4-week Step 1 review that maps your PHI flows, vendor stack, and technical controls, then hands back a regulatory-readiness read, before the first remediation check.
Five gaps that survive a green compliance dashboard
A green dashboard isn’t proof of anything. These five gaps pass a trust page and still get you caught in an OCR investigation or flagged in an enterprise security review, because they’re the first things both look for. For the fuller catalog, see our HIPAA compliance pitfalls guide; here are the five that survive a wall of checkmarks.
A spreadsheet of assumptions is not a risk analysis
Inadequate risk analysis turns up in roughly 90% of OCR Security Rule enforcement actions, the single most-enforced corner of the rule, and OCR enforcement is sharpening: the Risk Analysis Initiative now wants documented risk management on top of the analysis. What gets teams caught is treating a 20-minute spreadsheet of assumptions as the deliverable. A real risk analysis covers every system you mapped. You write it down, and you refresh it yearly. The civil monetary penalty range tells the story: settlements have run from $10,000 (Northeast Surgical Group) to $3 million (Solara Medical Supplies, the largest of 2025).
The BAA gaps hide in the vendors you forgot
“The vendor offers a BAA” and “you have a BAA” are different sentences, and three traps live in the gap.
- It’s gated behind a tier you’re not on. Mixpanel signs on Enterprise, Sentry on Business and up, Slack on paid plans, the LLM providers on their API or enterprise terms, never the consumer tier. On a free plan you’re uncovered. This is the real answer to ChatGPT HIPAA compliance, and the same logic runs through AI in healthcare compliance.
- The SDK leaks PHI by default. Error monitors like Sentry and Datadog grab URLs with patient IDs, request bodies, and stack-trace locals holding patient objects. Scrubbing configs reduce the exposure without removing the BAA requirement, and the leak stays invisible until an audit finds it.
- It won’t sign at any tier. Google Analytics, HubSpot, Meta, Contentsquare, Heap, Hotjar; and Firebase’s analytics piece isn’t covered by Google’s BAA even when the rest is. No tier fixes that, so de-identify before sending or switch. There’s no compliant workaround.
The cloud BAA covers their infrastructure, not your app
Signing the AWS HIPAA BAA feels like a finish line. It covers one thing: AWS’s infrastructure. The application on top of it is still yours to secure. Encryption, access controls, logging, and key management don’t transfer to the provider because you countersigned a document. We’ve audited teams who believed the platform’s BAA made them compliant; the app config underneath told a different story. The provider secures the building. You’re responsible for what you do inside it.
Audit logs are the first thing OCR asks for
When OCR opens an investigation, audit logs are close to the first thing they request, and enterprise buyers check for them in security review. Skipping them because they’re “not user-facing” is a common, expensive miss. Logs that count are tamper-evident and timestamped, and you retain them for as long as your policy says. A log you can quietly edit isn’t evidence, and an auditor knows the difference. Build them in early; reconstructing a year of access history after the fact runs from painful to impossible.
Compliance theater doesn’t survive an audit
Compliance theater is the gap that contains the other four. A trust page with green checkmarks. A template policy library nobody customized. A risk analysis someone finished over lunch. It photographs well and collapses the moment an auditor asks to see the control actually running. OCR’s 2026 posture is explicit: it targets documentation with no implementation behind it, and the documentation-as-defense era is closing. What holds up now is verifiable evidence that your controls run in production, the way the paperwork says. We see both versions in audits, and the gap between them is the whole ballgame.
Why Topflight Apps for HIPAA-compliant development
We build HIPAA-compliant digital health products from the ground up, with compliance in the architecture from the first commit. Here’s our actual lane, because it matters: we’re a technical and engineering compliance partner. We audit your product and build the HIPAA-compliant infrastructure (encryption, audit logging, BAAs) that gets you ready for SOC 2 Type II. The formal SOC 2 attestation and any legal opinion come from your auditor and your counsel; that’s their job, and we’ll tell you so.
The receipts: a decade building with healthcare startups, partners who’ve raised north of $200M, and real exits (Walker Tracker, acquired by Terryberry). This is our Vibe to Traction System lane, taking a working prototype to a secure, revenue-generating product. We’ve been through the audit conversation from prototype to SOC 2 readiness enough times to know the technical work that makes compliance hold up under a real audit, and what the gaps look like before and after a buyer’s security team digs in.
The teams that bolt compliance on after enterprise diligence flags it pay for the same work twice. So if you’re working out how to become HIPAA compliant and want an honest read on where you actually stand, and what it’ll cost to close the distance, talk to Topflight Apps. We know what buyers check, because we’ve sat on both sides of the table.
Frequently Asked Questions
How long does it take to become HIPAA compliant?
On HIPAA-eligible infrastructure from day one, a credible Year 1 program takes 4 to 6 months. SOC 2, if required, adds 3 to 6 months for the evidence period.
Do I need a HIPAA compliance officer?
Yes. HIPAA requires a designated Security Officer and Privacy Officer. At an early-stage startup that’s often one person, but you must put the designation in writing.
What AWS services are HIPAA-eligible?
It’s the most-enforced HIPAA requirement, appearing in roughly 90% of Security Rule actions. Settlements have ranged from $10,000 to $3 million.
What happens if I skip the risk analysis?
At mid-scale, yes, mostly because there’s no DevOps labor cost. AWS wins at high continuous-data volume, where Convex’s per-resource metering scales linearly while AWS reserved capacity stays flat. The crossover depends on your data access frequency, so model it at your real volume.
Can I use Google Workspace or Slack for PHI?
Only with a signed BAA. Google Workspace offers one; Slack offers one on paid plans. Neither is compliant by default; you still have to configure them to the BAA.