
If you’ve ever been through an HL7 or FHIR integration project, you know the drill: weeks of segment mapping, value-set reconciliation, edge-case testing, and debugging messages that look right but don’t behave right. It’s the kind of work that chews through timelines and budgets. So when someone says AI for HL7 FHIR integration can speed all of that up, the natural reaction is skepticism, and honestly, a little bit of hope.
The promise is real, but it’s not magic. AI can meaningfully accelerate parts of the integration process, particularly the repetitive, pattern-heavy work that eats up developer hours. But it can’t replace the domain expertise, clinical judgment, and system-level thinking that make healthcare integrations work safely in production.
This post breaks down where AI healthcare interoperability tools actually help, where they fall short, and how to decide if AI-assisted FHIR integration makes sense for your project.
| Can AI actually configure HL7 and FHIR integrations?
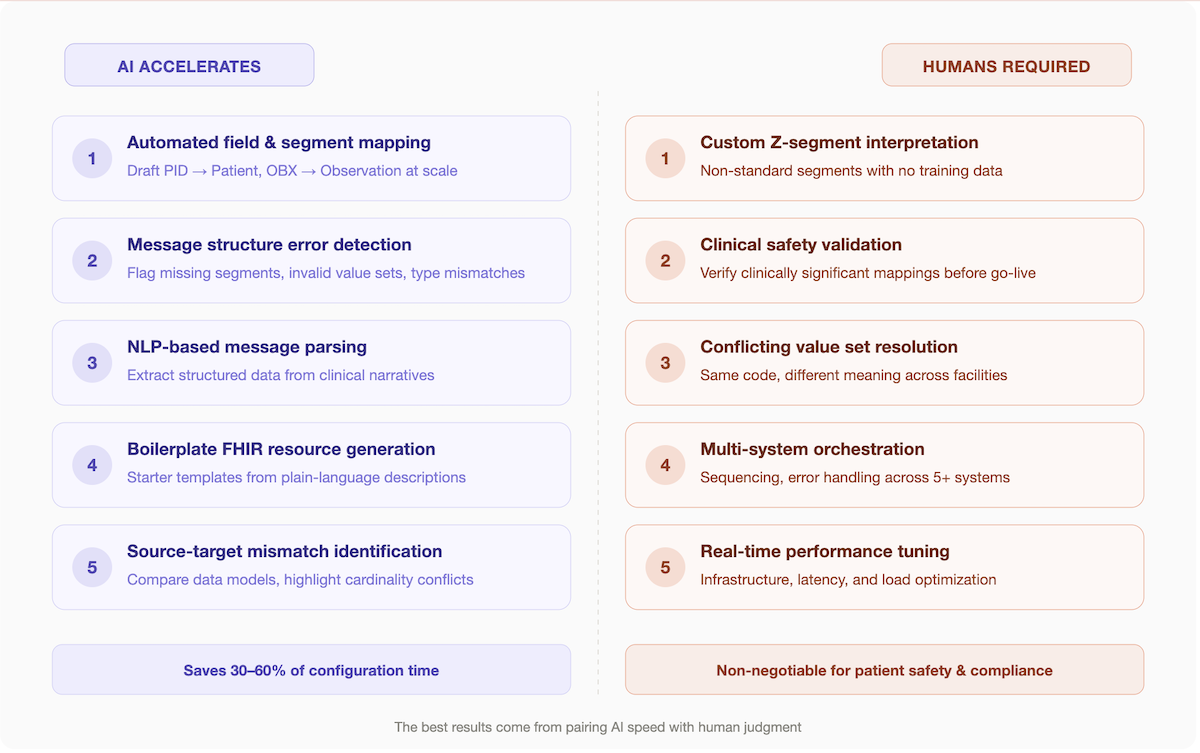
Yes but with limits. AI can automate field mapping, detect message structure errors, and generate boilerplate FHIR resource definitions, cutting integration configuration time by 30–60%. It cannot replace human review for clinically significant mappings, custom Z-segments, or multi-system orchestration. The best results come from pairing AI tooling with experienced integration developers. |
Key Takeaways
- AI cuts the busywork, not the expertise. Automated mapping, NLP-based parsing, and error detection can compress weeks of manual configuration into days but every AI-generated mapping still needs clinical validation before it goes to production.
- The ROI scales with volume. If you’re building a single interface, manual configuration may be faster. If you’re managing dozens of HL7/FHIR integration points across multiple systems, AI pays for itself by eliminating repetitive mapping and catching mismatches early.
- Tooling is ready but fragmented. AI-augmented integration engines, low-code FHIR platforms, and LLM-based mapping assistants all exist today. The challenge is picking the right combination for your EHR ecosystem, compliance requirements, and team capacity.
Table of Contents
- What Are HL7 and FHIR Integrations and Why Are They So Complex?
- How AI Can Help Configure HL7 and FHIR Integrations (the Honest Answer)
- Real-World Use Cases: Where AI Adds the Most Value in FHIR Integration
- What AI Still Cannot Do in HL7 / FHIR Integration (Don’t Oversell It)
- AI Tools and Platforms Supporting FHIR / HL7 Integration Today
- How to Evaluate Whether AI-Assisted Integration Is Right for Your Project
- Why Choose Topflight Apps for AI-Powered FHIR / HL7 Integration
- The Bottom Line: AI Is a Force Multiplier, Not a Replacement
What Are HL7 and FHIR Integrations and Why Are They So Complex?
Healthcare systems don’t naturally speak the same language. One hospital’s EHR might store lab results in a format that another hospital’s system can’t read without translation. That translation layer, the integration is where HL7 and FHIR come in.
HL7 v2 has been the workhorse of healthcare data exchange since the late 1980s. It uses pipe-delimited message segments (think PID for patient demographics, OBR for orders, OBX for observations) to move data between clinical systems. It works, but it’s notoriously flexible in the wrong ways: every implementation is slightly different, and those differences create HL7 message mapping headaches that can take days to untangle. HL7 v3 attempted to impose stricter data modeling with XML-based messages, but its complexity limited real-world adoption.
FHIR R4: Fast Healthcare Interoperability Resources is the modern answer. It uses RESTful APIs and modular data containers called FHIR resources (Patient, Observation, Condition, MedicationRequest, and so on) to structure clinical data exchange. FHIR is far more developer-friendly than its predecessors, but “more developer-friendly” doesn’t mean “easy.”
Here’s why these integrations are so hard to configure:
Segment and Field Mapping Is Inherently Ambiguous
The same clinical concept say, a patient’s allergies might live in different HL7 segments across different EHR systems. Mapping those to the correct FHIR AllergyIntolerance resource requires understanding both the source system’s idiosyncrasies and the target FHIR profile’s expectations. Healthcare data standards like SNOMED CT, LOINC, and ICD-10 add another layer of terminology mapping on top of structural mapping.
Versioning Differences Compound the Problem
A facility running HL7 v2.3 handles certain segments differently than one running v2.5.1. FHIR R4 and the incoming R6 have their own differences. An integration engine has to account for all of this.
The Cost of Getting It Wrong is High
A bad integration doesn’t just cause error logs, it can delay care. Mismatched medication codes can lead to wrong prescriptions showing up in a patient’s record. Dropped lab results can mean a critical diagnosis gets missed. And from a compliance standpoint, improperly handled data can trigger HIPAA violations and revenue leakage from rejected claims.
All of this explains why a single HL7-to-FHIR interface can take weeks to configure manually, and why organizations with dozens of integration points face timelines measured in months.
How AI Can Help Configure HL7 and FHIR Integrations
AI can meaningfully accelerate HL7 and FHIR integration configuration in several specific ways, but it does not replace domain expertise or testing.
The most impactful use cases are the ones where AI handles repetitive, pattern-based work while a human reviews the output and handles the edge cases. Here’s what’s actually working today:
Automated Field and Segment Mapping
Schema-aware AI models can analyze representative HL7 v2 messages and propose field-level data mapping to FHIR resources. For example, an AI system trained on healthcare data schemas can look at a batch of ADT (Admit-Discharge-Transfer) messages and automatically suggest
- how PID segments should map to FHIR Patient resources
- how PV1 segments map to Encounter resources
- how OBX segments map to Observation resources
This doesn’t eliminate mapping work but it can cut initial mapping time by 40–60% on straightforward interfaces.

NLP-Based Message Parsing and Transformation
Natural language processing can extract structured data from clinical narratives, discharge summaries, progress notes, free-text order descriptions and suggest how that data should be represented in FHIR. This is especially useful when migrating from older systems that store clinical information as unstructured text rather than discrete data fields.
AI-Assisted Error Detection
Instead of manually reviewing thousands of test messages for compliance issues, AI can scan HL7 message structures and flag problems: missing required segments, invalid value sets, data-type mismatches, and encoding errors. This catches issues earlier in the development cycle, before they reach production.
Boilerplate FHIR Resource Generation
Given a plain-language description of what a data pipeline needs to do, “map incoming lab results from the reference lab’s HL7 v2 feed into FHIR Observation and DiagnosticReport resources using LOINC codes” LLM-based tools can generate starter mapping templates, FHIR resource definitions, and even initial transformation logic. It’s not production-ready code, but it’s a useful starting point that saves hours of boilerplate work.
Mismatch Identification Between Source and Target Systems
AI can compare the data models of two systems and highlight where fields don’t align:
- different cardinality
- incompatible data types
- missing required elements
- conflicting code systems
This gives integration developers a prioritized list of problems to solve rather than having to discover them one by one during testing.
The key constraint is that AI still needs human review. Healthcare integration is a domain where a 95% accuracy rate isn’t good enough; the remaining 5% can affect patient safety, clinical workflows, or compliance status. AI-assisted configuration works best as a force multiplier for experienced integration developers, not as an autonomous system.

Real-World Use Cases: Where AI Adds the Most Value in FHIR Integration
The real test for any AI FHIR integration capability isn’t whether it works in a demo, it’s whether it holds up against the messy reality of production healthcare data. Here are the scenarios where AI delivers the most measurable impact.
EHR-to-EHR Data Migration
When a health system migrates from one EHR to another or when two organizations merge and need to unify their clinical data: EHR integration becomes a massive data translation exercise. The biggest bottleneck is mapping legacy HL7 v2 messages to FHIR R4 resources. Millions of historical records need to be translated, and each source system has its own quirks.
AI accelerates this by learning the mapping patterns from a representative sample of messages and then applying those patterns at scale. A model trained on the source system’s ADT, ORU, and ORM messages can generate draft mappings for the entire message library, which integration developers then validate and refine. For large migrations involving millions of patient records, this can compress what would be a 6-month mapping effort into 6–8 weeks.
Related: How to Integrate Your Medical App With EHR
This is also where AI’s ability to detect inconsistencies shines, it can flag records where the same patient appears with different identifiers, where medication codes don’t match across systems, or where lab units are incompatible.
Patient Data Onboarding
Healthcare organizations that aggregate data from multiple sources think health information exchanges, multi-practice groups, or digital health platforms face the challenge of normalizing incoming medical records from systems that all implement HL7 and FHIR slightly differently.
AI can classify incoming messages by type and source, apply the appropriate normalization rules, and flag records that don’t fit any known pattern for manual review. This is particularly valuable for organizations processing high volumes of data from dozens or hundreds of sending facilities, where manually configuring an interface for each one isn’t practical.
Compliance Monitoring
During integration configuration, certain data fields carry HIPAA-relevant implications: patient identifiers, social security numbers, dates of birth, and clinical notes all require specific handling. AI can audit integration configurations to flag fields that are being passed without appropriate de-identification, encryption, or access controls.
This doesn’t replace a formal HIPAA compliant software development review, but it catches obvious oversights before they become violations like a mapping that inadvertently exposes a patient’s SSN in a field that downstream systems treat as non-sensitive.
API Gateway Configuration
For organizations implementing SMART on FHIR applications, AI can recommend appropriate OAuth 2.0 scopes and access patterns based on the application’s intended functionality. If a third-party app needs read access to patient demographics and medication lists but not lab results, AI can suggest the minimal FHIR resource scopes needed, reducing the risk of over-permissioned API access.
This ties into the broader challenge of building HIPAA compliant app development pipelines where security isn’t bolted on after the fact but is part of the integration architecture from the start.
Understanding how will AI help change EHR systems at a structural level gives context for why these use cases matter, they’re not isolated improvements but part of a broader shift in how healthcare technology handles clinical data exchange and care coordination.
What AI Still Cannot Do in HL7 / FHIR Integration (Don’t Oversell It)
For all its genuine value, AI has clear limitations in healthcare integration work. Being honest about these limitations is important, overselling AI capabilities leads to failed projects, wasted budgets, and worse, clinical risk.
Custom Z-segments Remain a Manual Problem
HL7 v2 allows organizations to define custom segments (Z-segments) for data that doesn’t fit the standard schema. These are, by definition, non-standard, there’s no training data for an AI model to learn from. Every facility’s Z-segments are different, and mapping them requires direct conversations with the source system’s team to understand what each field means.
AI Cannot Guarantee Clinical Safety
An AI model might correctly map 98% of medication codes from a source system to the target FHIR MedicationRequest resource. But the 2% it gets wrong could include critical drugs with narrow therapeutic windows. Human validation of clinically significant mappings is non-negotiable. No responsible integration team should deploy AI-generated mappings to production without thorough clinical review.
Ambiguous and Conflicting Value Sets Are a Persistent Challenge
Different facilities often use the same code to mean different things, or different codes to mean the same thing. AI can flag potential conflicts, but resolving them requires domain expertise and often direct communication with clinical stakeholders at each facility. This is fundamentally a human judgment problem.
Complex Multi-System Orchestration Is Beyond Current AI Capabilities
When an integration workflow involves coordinating data flows across five or six systems, an EHR, a lab information system, a pharmacy system, a billing platform, a patient portal, and a health information exchange, the sequencing, error handling, and fallback logic require an integration architect who understands the full system landscape. AI can assist with individual point-to-point mappings, but it can’t design the overall data pipeline architecture.
Real-Time Performance Constraints Are Hard for AI to Reason About
An integration that works perfectly in a test environment might fail under production load if it’s processing thousands of messages per minute. AI tools today don’t have visibility into infrastructure constraints, network latency, or database performance characteristics. Tuning an integration for real-time clinical data exchange still requires hands-on engineering.
AI Tools and Platforms Supporting FHIR / HL7 Integration Today
The market for AI-augmented healthcare integration is maturing but still fragmented. Here are the main categories of tools worth evaluating:
AI-Augmented Integration Engines
Traditional integration engines like Rhapsody and Mirth Connect (now NextGen Connect) are the backbone of most healthcare integration operations.
Newer AI plugins and extensions are adding capabilities like automated mapping suggestions, message validation, and anomaly detection on top of these established platforms. The advantage is that teams can add AI assistance without replacing their existing infrastructure.
Low-Code FHIR Platforms with AI Features
Platforms like Firely, Azure Health Data Services, and Kodjin offer FHIR server infrastructure with built-in tooling that increasingly includes AI-assisted mapping and validation. Azure Health Data Services in particular benefits from Microsoft’s broader AI investments, offering FHIR conversion, de-identification, and analytics capabilities in a managed cloud interoperability platform.
LLM-Based Mapping Tools and Integration Assistants
A growing number of vendors and open-source projects are using large language models to assist with FHIR resource generation, HL7 message parsing, and terminology mapping. These tools are useful for generating starter configurations and exploring mapping options, though their output consistently requires expert review. Questions about ChatGPT HIPAA compliance are relevant here, any tool that processes real patient data during configuration needs to meet healthcare privacy requirements.
Custom AI Layers on Top of Existing Middleware
For organizations with complex integration landscapes, the most effective approach is often building a custom AI layer that sits on top of existing middleware. This allows teams to train models on their specific data patterns, source system quirks, and organizational terminology preferences something off-the-shelf tools can’t fully replicate.
Topflight builds custom AI-powered integration layers tailored to specific EHR workflows combining deep healthcare domain expertise with practical AI implementation to accelerate integration timelines without compromising clinical safety or compliance. The cost of AI in healthcare projects varies significantly based on scope, but the ROI from reduced integration time and fewer production errors is measurable.
How to Evaluate Whether AI-Assisted Integration Is Right for Your Project
Not every integration project needs AI and not every project is ready for it. Before you configure HL7 FHIR with AI tooling, here’s how to assess fit:
Volume and Complexity of Message Types
If you’re building a single HL7 interface between two well-documented systems, manual configuration might be faster than setting up an AI-assisted workflow. AI shows its value when you’re dealing with dozens of interfaces, high message volumes, or legacy systems with poorly documented data models.
Existing Infrastructure and EHR Systems Involved
The major EHR vendors Epic, Cerner (now Oracle Health), and Athenahealth, all have their own integration patterns and APIs. AI tools that are trained on or optimized for specific EHR ecosystems will be more effective than general-purpose mapping tools. Understanding your current stack determines which AI approach makes sense. For Athenahealth environments, Athena EMR/EHR integration should be planned around vendor-specific API behavior, data mapping rules, authentication requirements, and validation workflows before introducing AI-assisted configuration.
Team’s Technical Capacity
AI-assisted integration still requires people who understand HL7, FHIR, and clinical data flows. If your team has that expertise, AI can make them faster. If you’re starting from scratch, AI alone won’t compensate, you’ll need either experienced in-house integration developers or a partner with deep healthcare interoperability experience.
Regulatory and Compliance Requirements
HIPAA, ONC certification requirements, and CMS mandates (including the CMS Interoperability and Prior Authorization Final Rule requiring FHIR-based APIs by 2027) all affect how integrations must be designed, tested, and documented. AI tools can help generate compliance documentation and audit trails, but the underlying compliance architecture needs to be designed by people who understand the regulatory landscape.
The intersection of AI and healthcare data is also relevant in adjacent areas like AI in medical billing and coding and conversational AI in healthcare, where similar principles of automation with human oversight apply.
Why Choose Topflight Apps for AI-Powered FHIR / HL7 Integration
Topflight combines hands-on experience with FHIR R4 and HL7 v2 integration, deep familiarity with major EHR platforms like Epic and Cerner, and a practical approach to applying AI where it actually accelerates results.
We build HIPAA-compliant integration architectures that use AI for the tasks it handles well automated mapping, validation, error detection, and test data generation, while keeping experienced integration engineers in the loop for clinical review, edge-case handling, and production deployment.
Whether you’re migrating legacy HL7 interfaces to FHIR, building a new healthcare API layer, or connecting a digital health product to existing clinical systems, Topflight can help you scope, build, and deploy AI-powered FHIR integration solutions that work in the real world.
The broader applications of gen AI in healthcare are expanding rapidly, and integration infrastructure is the foundation that makes everything else possible.
Talk to a Healthcare Integration Expert →
The Bottom Line: AI Is a Force Multiplier, Not a Replacement
AI is a genuine accelerator for HL7 and FHIR integration, especially for mapping, validation, error detection, and boilerplate generation. HL7 FHIR integration automation reduces the time integration developers spend on repetitive tasks and catches issues earlier in the development cycle.
But it’s not a replacement for expertise. Custom Z-segments still need human interpretation. Clinically significant mappings still need clinical review. Multi-system orchestration still needs architectural thinking. And compliance still needs people who understand the regulatory environment.
The smart move is pairing AI tooling with experienced integration developers who know healthcare data standards inside and out. That combination: AI speed with human judgment is where the real value lives.
Frequently Asked Questions
Can AI automatically map HL7 v2 messages to FHIR R4 resources?
AI can generate draft mappings between HL7 v2 segments and FHIR R4 resources by analyzing message structures and applying learned patterns from healthcare data schemas. However, these mappings require human validation before production use, particularly for clinically significant fields where errors could affect patient care or regulatory compliance.
What is the difference between HL7 and FHIR, and how does AI handle both??
HL7 v2 is a legacy messaging standard that uses pipe-delimited segments (like PID, OBR, OBX) for clinical data exchange. FHIR is the modern successor, using RESTful APIs and modular resources (Patient, Observation, Condition) based on web technologies. AI tools can work with both standards, parsing HL7 v2 messages, generating FHIR resource mappings, and identifying structural mismatches between the two. The challenge is handling the variability in how different organizations implement each standard.
Is AI-assisted FHIR integration HIPAA compliant?
AI-assisted integration can be HIPAA compliant, but it depends entirely on implementation. The AI tools themselves must handle protected health information (PHI) within a HIPAA-compliant environment, meaning proper encryption, access controls, audit logging, and business associate agreements. Using a general-purpose AI model to process real patient data without these safeguards would violate HIPAA. Organizations should evaluate any AI integration tool against the same HIPAA development standards they apply to any other system that touches PHI.
How long does it take to configure an HL7/FHIR integration with AI tools?
Timelines vary based on complexity, but AI-assisted configuration can reduce integration development time by 30–60% compared to fully manual approaches. A straightforward single-interface HL7-to-FHIR mapping that might take 4–6 weeks manually could be completed in 2–3 weeks with AI assistance. Complex multi-system integrations still take months, but AI compresses the mapping and validation phases significantly.
What types of healthcare systems benefit most from AI-powered FHIR integration?
Can small healthcare organizations afford AI-assisted integration tools?
Many AI-assisted integration capabilities are becoming available through existing platforms at moderate cost: tools like Mirth Connect with AI plugins, or cloud-based FHIR services from Azure or Google Cloud that include AI features in their standard pricing. Smaller organizations may not need the custom AI layers that enterprise health systems build, but they can still benefit from AI-powered mapping suggestions and validation built into the platforms they’re already using.
Does AI-assisted integration work with Epic, Cerner, or Athenahealth?
Yes. AI-assisted integration tools are EHR-agnostic at the protocol level: they work with HL7 v2 messages and FHIR APIs regardless of which EHR generates them. That said, each EHR vendor has specific implementation patterns, API quirks, and certification requirements. Epic’s FHIR APIs follow the Argonaut/US Core profiles, Cerner (Oracle Health) has its own FHIR implementation guide, and Athenahealth uses a combination of proprietary APIs and FHIR endpoints. AI tools trained on or configured for specific EHR ecosystems will produce more accurate mapping suggestions out of the box.