
Most rehab products fail quietly: patients stop following the plan, therapists don’t trust the data, and the app turns into a “nice-to-have” that lives outside the real workflow. Rehab app development only works when you build around the clinical loop—assignment → execution → feedback → adjustment—and make that loop easier than doing rehab without the app.
This guide breaks down the app types that win (and why), the features that actually drive adherence, the architecture behind motion tracking and remote monitoring, and the compliance/integration choices that keep you deployable in real healthcare settings.
Key Takeaways
- Adherence is the product. If your app doesn’t reduce confusion (“what do I do today?”) and make progress visible, you’ll lose users long before you lose them to a competitor.
- Workflow beats features. The fastest growth lever is a therapist dashboard that enables triage and quick plan edits—not another patient-facing widget.
- Integrations decide adoption. EHR connectivity, billing-ready reporting, and reliable device data separate “pilot apps” from systems clinics keep using.
Understanding Rehabilitation App Development in Modern Healthcare

What Rehabilitation Apps Are and Their Role in Recovery
At a practical level, rehabilitation app development is about turning therapy from a “see you next week” event into a continuous loop: guided sessions at home, clear instructions, and enough feedback that people actually do the work.
The best apps don’t try to replace clinicians. They remove friction around patient recovery: what to do today, how to do it safely, and whether you’re progressing or compensating (aka “cheating” with the wrong muscles).
This is where rehabilitation technology stops being a buzzword and becomes infrastructure: remote guidance, tracking, clinician oversight, and tight feedback loops that make adherence more likely and outcomes measurable.
Market Growth and Demand for Digital Rehabilitation Solutions
If you want a reliable growth signal without stretching definitions: the telerehabilitation market (a major slice of “digital rehab”) was estimated at $5.32B in 2024 and projected to reach $11.81B by 2030, implying about 13.2% CAGR (2025–2030).
That demand is being pulled by exactly what you’d expect: more remote care, more chronic conditions, and the simple fact that people prefer rehab that fits into life, not the other way around.
Types of Rehabilitation Apps: Physical, Occupational, and Speech Therapy
Instead of forcing a too-neat PT/OT/speech “market share pie chart,” it’s more accurate to think in use-case buckets:
- Orthopedic / MSK rehab (post-op and injury recovery): commonly cited as one of the largest segments; one telerehab market breakdown lists orthopedic applications at 31.9% (2024).
- Neuro rehab (stroke, movement disorders): higher complexity, often longer programs and more caregiver involvement.
- Cardio/pulmonary rehab: strong fit for remote monitoring plus coaching.
- Speech/OT-focused programs: often narrower features, but high value when paired with clinician workflows.
On the product side, software tends to dominate the spending: the same telerehab breakdown estimates the software segment at 60.2% (2024)—which lines up with where the hard work lives (workflows, content, analytics, clinical tooling).
Benefits for Patients, Therapists, and Healthcare Organizations
The benefit story gets real when you talk in measurable rehabilitation outcomes rather than vibes:
- Adherence: a review summarizing a systematic review/meta-analysis reports digital rehab adherence averaging ~65–85%, compared with ~40–60% in conventional programs. That’s not a “nice-to-have”—it’s the whole game.
- Utilization/readmissions: in cardiac rehab, a cohort study of a virtual program reported lower 1-year all-cause readmissions (incidence rate ratio 0.616, ~38% lower vs comparator).
- Clinical scalability: when routine check-ins and progress review move into a therapist dashboard, clinicians spend less time “chasing updates” and more time adjusting care.
This is also where digital therapeutics thinking matters: the app isn’t “content.” It’s a delivered intervention—meaning you design for engagement, measurement, and iteration like it actually has to work in the wild (because it does).
Types of Rehabilitation Apps: Comprehensive Overview
A rehabilitation app (including a physical rehabilitation app) can mean anything from a protocol-driven recovery companion to a full telerehab platform. The fastest way to choose the right direction is to map the app type to the rehab loop you’re supporting:
- teach the right movement
- monitor execution and symptoms
- adjust the plan before patients drift off course
This is where rehab differs from fitness app development—you’re not optimizing for “more,” you’re optimizing for safe, measurable progress.
Physical Therapy and Musculoskeletal Rehabilitation Apps
Orthopedic Recovery Applications
These apps are built around procedure-specific pathways:
- joint replacements
- ACL reconstruction
- rotator cuff repair
- spine recovery
The product is structured—clear phases, contraindications, and progression rules—so patients can follow a plan that aligns with real-world physical therapy workflows. This category is the core of post-surgical rehabilitation, because the plan is known, but adherence and execution are fragile.
Sports Injury Rehabilitation Apps
For sports injury recovery, the app has to do more than count reps. It should support return-to-play logic:
- progressive loading
- sport-specific drills
- performance tracking
- injury-prevention routines
The differentiator is decision support: are we ready to progress, or is the athlete compensating, inflamed, or simply overdoing it?
Chronic Pain Management Apps
Chronic pain management isn’t “PT with a pain slider.” These apps blend movement therapy with pacing, education, and often CBT-style modules and mindfulness.
Pain tracking matters, but context matters more—what activity triggered the flare, what helped, what patterns repeat—so clinicians can coach behavior, not just react to symptoms.
Neurological Rehabilitation Applications
Stroke Recovery Apps
Stroke rehabilitation apps often span motor retraining, cognitive exercises, and daily living activities—and they frequently intersect with speech therapy needs (aphasia, dysarthria). They work best when the app supports high-frequency practice, simple feedback loops, and caregiver involvement.
Traumatic Brain Injury (TBI) Apps
TBI rehab tends to focus on attention, memory, executive function, and routine building. The key product principle is adaptive load: short sessions, flexible progression, and monitoring that recognizes good and bad days without punishing variability.
Parkinson’s and Movement Disorder Apps
These apps combine gait and balance training with symptom tracking and reminders. They’re less about “perfect form” and more about consistency: the right work at the right time, with data clinicians can actually use.
Cardiopulmonary Rehabilitation Apps
Cardiac Rehabilitation Programs
Cardiac rehab apps guide exercise progression and lifestyle education while monitoring intensity (heart rate, perceived exertion) and adherence. They’re designed to keep patients engaged and safe outside the clinic.
Pulmonary Rehabilitation Apps
Pulmonary rehab apps emphasize breathing exercises, pacing, symptom tracking, and education—sometimes supported by oxygen saturation monitoring—so patients build capacity without spiraling into avoidance.
Specialized Therapy Applications
Pediatric Rehabilitation Apps
Pediatric rehab succeeds with gamification, parent involvement, and milestone tracking. The “user” is often a parent-coach plus a child, so routines and rewards matter as much as content.
Geriatric Rehabilitation Apps
Geriatric rehab apps prioritize safety and simplicity: fall-prevention programs, cognitive supports, medication management, and confidence-building through steady progress.
Occupational Therapy Apps
Occupational therapy apps focus on activities of daily living, workplace ergonomics, adaptive techniques, and fine motor skill training—because “function” is the outcome.
Speech and Language Therapy Apps
Beyond articulation practice, speech apps can include language comprehension, voice therapy, swallowing exercises, and guided home assignments tracked over time—often as part of a broader rehab plan.
Telerehabilitation Platforms
Comprehensive Virtual Therapy Suites
These platforms unify multi-disciplinary care: video sessions, secure messaging, remote assessments, and shared treatment plans across teams.
Remote Patient Monitoring Apps
RPM-first solutions add continuous tracking, automated alerts, and clinician dashboards to drive timely intervention and outcome reporting—especially valuable when patients are remote and caseloads are large.
Not sure which type of rehabilitation app fits your needs? Our experts will help you choose the right solution.
Essential Features for Rehabilitation Apps
If you want to create a rehabilitation app that patients actually use—whether you’re trying to create a physical therapy app or a multi-discipline program— don’t start with “AI posture correction.” Start with the boring stuff that makes rehab work: clarity, routine, feedback, and a plan that adapts when real life happens.
The best patient engagement apps in rehab feel like a coach that’s always available—without feeling like homework. In practice, ‘sessions’ can mean therapeutic exercises, breathing work, speech drills, cognitive tasks, or daily-living routines—depending on the discipline.

Patient-Side Features for Engagement and Recovery
Exercise Library with Video Demonstrations
Your exercise library is the product—a curated set of therapeutic exercises. Everything else is plumbing. It needs:
- crisp video demonstrations (HD, multiple angles)
- optional 3D cues
- step-by-step safety notes
- “what it should feel like vs what it shouldn’t.”
Patients don’t fail because they’re lazy; they fail because they’re unsure. Good home exercises remove ambiguity.
Progress Tracking and Analytics
This is where trust gets built. Patients should see progress tracking that’s simple and motivating:
- pain trends
- streaks
- weekly volume
- functional checkpoints
Clinically, you want exercise tracking tied to metrics that matter—range of motion, strength checks, and symptom response—so progress monitoring isn’t just a pretty chart; it’s evidence that the plan is working (or not). Done right, you’re not “tracking for tracking’s sake,” you’re building accountability and confidence.
Real-Time Feedback and Form Correction
Real-time cues are useful, but only when they’re reliable and humble. Start with practical guidance (rep counting, tempo cues, posture reminders) and graduate to motion detection when accuracy is good enough to avoid false alarms.
Gamification and Motivation Systems
Yes, gamification works—when it reinforces recovery, not ego. Streaks, badges, and milestones should reward consistency, not intensity. Pair it with lightweight patient engagement hooks:
- Micro-goals
- “today’s win”
- reminders that feel supportive, not naggy
People don’t need more pressure; they need a plan that fits their day.
Therapist Dashboard and Clinical Tools
Treatment Plan Creation and Customization
A rehab app without strong clinician tooling becomes a content library with delusions of grandeur. A therapist dashboard must make it fast to build and adapt treatment plans:
- protocol templates
- patient-specific modifiers
- a clean exercise prescription workflow
If it takes longer than doing it manually, therapists won’t adopt it.
Patient Monitoring and Intervention
This is the “save the program” layer: compliance flags, symptom spikes, missed sessions, and escalation triggers. Tie patient compliance to interventions that are actually actionable—message the patient, adjust dosage, swap an exercise, schedule a check-in—plus optional medication reminders when they’re part of the recovery plan.
And because rehab is often multidisciplinary, bake in care team collaboration (shared notes, handoffs, role-based visibility) so the app doesn’t create silos.
Outcome Measurement and Reporting
You need outcome measures that satisfy both clinical reality and operational needs: standardized functional scores, ROM logs, and documentation that supports payer conversations when applicable.
Advanced Features Using AI and Machine Learning
Computer Vision for Movement Analysis
When it’s mature, computer vision can detect compensations and form drift, especially for simple movements. But treat it as “assistive,” not authoritative—patients and clinicians need transparent feedback, not black-box scoring.
Predictive Analytics for Recovery Optimization
This is the big unlock: using adherence patterns, symptom trends, and session history to predict risk and personalize progression. If you can forecast likely drop-off, you can intervene early—with smarter prompts, plan adjustments, or timely appointment scheduling for remote therapy check-ins before the patient disappears.
Technical Architecture for Rehabilitation Apps
To develop rehabilitation software that clinicians trust and patients can’t accidentally “game,” you need an architecture that treats measurement as a first-class feature — not just in rehab, but across healthcare apps in general, as outlined in this healthcare mobile app development guide.

Choosing the Right Technology Stack
Mobile Development: Native vs. Cross-Platform
If your roadmap includes real-time motion tracking (form cues, rep counting, joint-angle estimation), native iOS/Android tends to win on camera performance, sensor access, and latency control.
If your initial scope is mostly content + logging + messaging, cross-platform (React Native/Flutter) is often the pragmatic path—faster iteration, shared UI logic, and simpler maintenance.
A useful rule: build the “app shell” cross-platform, but keep a lane open for native modules when you introduce heavier sensing, computer vision, or anything that needs tight frame-by-frame control.
Backend Infrastructure for Healthcare Data
Rehab apps generate messy streams: sessions, adherence events, symptom logs, and sometimes high-frequency signals from sensors. Your backend has to handle:
- scalable storage for time-series data (sessions and signals),
- near-real-time processing for alerts and dashboards,
- and clean separation between “identity/auth” and clinical data domains.
In non-motor programs, the high-signal stream is often patient-reported outcomes, short assessments, and adherence patterns—not camera data.
If you want real value from data analytics, design the event model early: every session should produce structured events (started, completed, modified, stopped, pain-spike, form-warning). Otherwise your dashboards become vibes-based.
Integration with Medical Devices and Wearables
This is where wearable app development and reality collide. Wearable devices don’t just “connect”—they drop packets, vary by firmware, and disagree on units. Expect to support:
- Bluetooth LE for rehab sensors and peripherals,
- API-based ingestion (Apple Health/Google Fit and device vendors),
- and a normalization layer that turns chaos into consistent biometric data (heart rate, steps, HRV where available, SpO₂ in some setups).
When you step into medical device integration, treat device data like an external clinical source: version it, validate it, and log provenance (“from which device, which firmware, which timestamp model?”). That’s how you avoid debugging by séance later.
Motion Tracking and Analysis Technologies
Camera-Based Motion Capture
Camera-first approaches are attractive because they’re frictionless: no hardware, just a phone. Under the hood, you’ll rely on pose estimation pipelines (commonly via frameworks like MediaPipe-style stacks) and build guardrails for lighting, occlusion, and camera placement.
This is the gateway to AI assessment: “your knee is collapsing inward” is useful only if you can explain it and it’s accurate enough not to annoy users into uninstalling.
When you need deeper fidelity—joint angles, symmetry, compensation patterns—camera pipelines can evolve toward 3D motion analysis, but that raises cost and complexity fast:
- compute
- calibration assumptions
- edge cases
Sensor Integration and Wearable Devices
Sensors shine when the camera struggles: off-angle views, tight spaces, or movements where inertial signals are more reliable than pixels. Common stacks include IMUs (accelerometer/gyroscope), pressure sensors, and sometimes EMG.
The real work is data fusion: combining signals into stable features that clinicians can interpret.
Data Security and HIPAA Compliance
Even the cleanest architecture fails if it can’t protect patient data. Build for:
- end-to-end encryption in transit, and strong encryption at rest,
- secure authentication and role-based access,
- audit trails for access and changes,
- and data minimization/anonymization where feasible.
Operationally, your compliance posture depends on vendors too: hosting, analytics tooling, messaging, video, and device platforms all become part of the risk surface.
Finally, if your product leans on machine learning, treat model inputs/outputs as part of the clinical record: log versions, keep explainability artifacts where possible, and ensure your pipeline can be audited. In rehab, “the model said so” isn’t a feature—it’s a lawsuit draft.
Development Process and Implementation Timeline
If you want to build a rehabilitation app that survives contact with real clinics (and real humans), don’t plan it like generic healthcare app development. Rehab is outcomes-driven: you’re not shipping “features,” you’re shipping behavior change plus clinician workflow. That changes how you sequence work, what you validate early, and where you spend time.
Phase 1: Discovery and Requirements Analysis (4–6 weeks)
This is where you decide what you’re actually building—and what you’re deliberately not building yet. Do stakeholder interviews (therapists, ops, compliance, and a few patients), map the current workflow, and define the clinical loop: assignment → execution → feedback → adjustment.
Deliverables that matter:
- product goals tied to measurable recovery milestones (not “engagement” in the abstract),
- a data model for sessions, symptoms, and adherence,
- risk + regulatory assessment (HIPAA baseline, device/data sources, any SaMD implications),
- and a realistic MVP scope that clinicians won’t laugh at.
Phase 2: UX/UI Design for Accessibility (6–8 weeks)
Rehab apps live or die on usability. Patients use them when they’re tired, sore, stressed, or older. Design around that reality:
- user journey mapping for both patient and therapist flows,
- WCAG-aware UI choices (contrast, touch targets, readable typography),
- usability testing with the least “tech-savvy” users you can recruit (that’s the honest test),
- and a design system that supports fast iteration without UI drift.
The key: every screen should answer one question quickly—“what do I do now?”—because confusion kills treatment adherence faster than lack of motivation.
Phase 3: MVP Development and Core Features (12–16 weeks)
Build the core loop end-to-end before you get fancy:
- exercise library + assignment flow,
- basic tracking (completed sessions, pain/symptom notes),
- therapist dashboard essentials (create plans, review progress, message/check-ins),
- authentication, roles, audit logging, and initial QA.
A good MVP proves three things: patients can complete sessions, therapists can adjust plans without friction, and your data is trustworthy enough to support decisions.
Phase 4: Advanced Features and AI Integration (8–12 weeks)
Only after the MVP loop works should you layer in complexity:
- motion analysis and form feedback,
- wearable integrations,
- advanced analytics and risk flags (drop-off predictors, stalled progress signals).
Treat AI as assistive: it should reduce clinician workload and improve feedback, not create a second system clinicians must babysit.
Phase 5: Clinical Validation and Testing (6–8 weeks)
This phase is about credibility and safety:
- validate outcome metrics and progression logic with clinicians,
- run structured usability studies,
- test edge cases (missed sessions, pain spikes, wrong exercise execution),
- iterate on the thresholds that trigger outreach or plan changes.
This is also where you tighten your milestone definitions: what counts as progress, what counts as regression, and what interventions are appropriate at each stage.
Phase 6: Launch and Post-Launch Support
Launch is a beginning, not a finish line:
- app store submission + onboarding flows,
- performance monitoring (crashes, latency, sensor reliability),
- feature updates based on real adherence patterns,
- support processes for clinics and patients.
Post-launch, you’ll usually find that the biggest wins come from small tweaks: better reminders, clearer instructions, and smarter escalation when adherence drops—because the product’s job is to keep patients moving toward the next milestone, not just to exist on their phones.
Cost Analysis for Rehabilitation App Development
Cost estimates in rehab app development only get useful when you anchor them to three things:
- What patients do in the app.
- What therapists do in the dashboard.
- Which integrations or sensing features you’re betting on.
Below are planning bands by product tier—plus the drivers that reliably move you up.
MVP Development Costs by App Type
Basic Exercise Tracking App
Planning band: ~$50k–$100k+ for a telehealth-style MVP scope.
What’s typically included: exercise library, basic tracking (sessions completed, pain notes), simple therapist portal, authentication/roles, baseline security and auditing.
What’s usually not included yet: sophisticated analytics, deep integrations, motion analysis, multi-clinic admin tooling, complex reporting.
A good heuristic: if your MVP is “assign exercises → patient completes → therapist reviews and tweaks,” you’re in this tier—unless integrations force you out of it.
AI-Powered Motion Analysis Platform
This tier isn’t expensive because “AI is cool.” It’s expensive because you’re building (and testing) a measurement system in messy home conditions.
Planning signal from CV cost guides: custom computer-vision builds are often cited in the ~$100k–$350k total range, with MVPs starting around ~$80k (for the CV layer + product integration), depending on scope and data approach.
What’s typically included (beyond tracking MVP): camera/sensor pipelines, QA for device variance and edge cases, clinician-safe feedback UX, and tooling for calibrating/iterating the model logic.
Comprehensive Telerehabilitation Suite
Planning band: many telemedicine cost guides cite ranges like ~$40k for a basic MVP up to $400k+ for feature-rich/enterprise solutions.
The reason suites trend toward the high end isn’t “more screens.” It’s workflow complexity + integrations + governance.
What’s typically included: multi-role admin, messaging, scheduling, video visits, richer therapist workflow, multi-program support, reporting, and (often) one or more major integrations.
Video as a concrete add-on: one estimate puts a HIPAA video consult feature (e.g., Twilio-based) around $8k–$15k to implement. Note that it’s not the whole suite cost—just a useful “known chunk.”
Factors Affecting Development Costs
- Platforms + roles: patient + therapist + admin across iOS/Android/web multiplies build + QA.
- Integrations: EHR, billing, wearables, device vendors—each one is its own project with long-tail support cost.
- Compliance/security scope: auditability, vendor governance, logging, access controls, retention rules.
- AI/sensing depth: camera pipelines, sensor fusion, validation, and the “false alert” problem.
- Clinical validation + content operations: protocols, exercise content quality, and iteration cycles with clinicians.
ROI and Revenue Models
Common models include B2B clinic licensing (per clinic/provider), enterprise agreements, payer/employer programs, and—in some programs—reimbursement-aligned pathways (where your product and documentation must match the requirements).
The ROI story usually hinges on measurable adherence and operational efficiency: fewer drop-offs, earlier interventions, and less manual follow-up.
If you share your target rehab use case and the integrations you need (video, EHR, wearables, billing), we can map it to one of these tiers and give you a scoped estimate with tradeoffs spelled out—what to ship in the MVP, what to defer, and what will increase cost no matter what.
Regulatory Compliance and Clinical Validation
In therapy app development, compliance isn’t a checklist—it’s the set of constraints created by your claims, your data flows, and whether clinicians can reasonably rely on your outputs. You already have the technical hygiene covered; the real risk now is building something that can’t be deployed, reimbursed, or defended.
FDA and SaMD: the “Claim Boundary” Is the Product
Your fastest path to trouble is shipping features that behave like clinical decision-making while marketing them like “wellness.” If you’re delivering digital therapeutics-style guidance or dosing progression, treat “intended use” as a design artifact: what the app does and what it implies.
- If the app’s recommendations affect diagnosis/therapy decisions, you’re in Software as a Medical Device territory and may be pulled toward 510(k) expectations (depending on risk and predicate landscape).
- For ML features, the compliance pain isn’t the model—it’s change control: how updates are validated, versioned, and rolled back when outcomes drift.
HIPAA: Stop Treating It Like a Security Spec
HIPAA compliance lives in operations: access is necessary but not sufficient. HIPAA compliant development means you can explain (and prove) who accessed what, why they were allowed, what vendors touched it, and how incidents are handled. The “gotchas” in rehab are usually:
- multi-role visibility (patient/therapist/admin/caregiver),
- communications surfaces (video, messaging, file uploads),
- and analytics tooling that quietly becomes PHI processing.
Clinical Evidence: Validate the Protocol, Not the UI
The credibility question is: do outcomes improve because the app enforces clinical logic? Tie validation to clinical protocols and the metrics clinicians/payers care about: functional scores, standardized PROMs, ROM-based measures where relevant, and adherence as a mediator, not the endpoint.
If your product claims superiority, you need study design discipline (comparators, blinding where possible, clear endpoints) and an audit trail of protocol changes. That’s how you defend evidence-based therapy rather than “we shipped features.”
International and standards: build once, document twice
If Europe is on the roadmap, plan for CE marking pathways, quality system expectations (often aligned with ISO 13485 for regulated products), and GDPR’s practical constraints (lawful basis, data minimization, retention, patient rights). The cost isn’t paperwork—it’s rework when documentation and product reality don’t match.
Integration with Healthcare Ecosystem
In telerehabilitation app development, integrations aren’t “nice-to-have add-ons.” They decide whether your product becomes part of care delivery—or just another app patients forget exists.
The goal of healthcare integration is simple: reduce double documentation, keep clinicians in their workflow, and make outcomes/reporting defensible.

EHR/EMR Integration Strategies
EHR integration succeeds when you’re brutally specific about what you’re integrating and why. Start by choosing one of three patterns (and don’t pretend you’re doing all three on day one):
- Read-only context pull (lowest risk): patient demographics, problem list, appointments, care team. Great for “right patient, right plan” and reduces manual entry.
- Write-back of discrete outcomes (higher value, higher risk): session completion, selected outcome measures, key observations. This is where EHR connectivity gets political—clinicians will ask “what becomes part of the legal record?”
- Orders/tasks loop (highest operational impact): referral → plan assignment → progress review → discharge summary. This is where integration becomes workflow.
Yes, HL7 FHIR is the lingua franca, but the hard part is data mapping + identity: patient matching, encounter context, and reconciling duplicates. Real-time sync is rarely “real-time”; design for eventual consistency, retries, and reconciliation logs so you can prove what happened when something goes missing.
Insurance and Billing Integration
If you’re touching reimbursement, “export a PDF” isn’t an integration strategy. Insurance billing work usually breaks down into:
- capturing the right operational signals (time, frequency, device usage if applicable, clinician involvement),
- mapping those to CPT/HCPCS logic your customers actually use,
- and producing artifacts that survive audits (who did what, when, and under which protocol).
Prior auth and claims submission can be integration-heavy (clearinghouses, payer portals, RCM systems). A pragmatic MVP approach: start with “billing-ready data + documentation outputs” before you attempt end-to-end claims automation.
Connecting with Wearables and IoT Devices
Wearables aren’t one integration—they’re an ecosystem. Apple HealthKit and Google Fit can cover baseline signals, while device APIs add richer streams. The non-obvious requirement is standardization: normalize timestamps, units, sampling rates, and provenance. Without that, your analytics and clinician trust both collapse.
Telemedicine Platform Integration
Most teams assume video is the main task. It isn’t. The real telehealth integration problem is coordinating: scheduling, secure messaging, consent flows, care team visibility, and follow-ups.
In telehealth app development, video should be a swappable component (vendor-agnostic), while the workflow glue—notifications, routing, documentation hooks—is what makes it stick.
Rule of thumb: integrate where it removes clinician work. If an integration doesn’t reduce clicks or documentation burden, it’s usually just an expensive checkbox.
Best Practices and Success Factors
Most recovery app development fails for one of two boring reasons: patients don’t stick with it, or clinicians won’t adopt it. Everything below is designed to protect patient adherence and clinician sanity—because you rarely get one without the other.
User Engagement and Retention Strategies
Don’t “motivate.” Reduce friction and make progress obvious.
- Personalize the plan, not the marketing. “Do these 3 exercises today” beats generic encouragement. Personalization should mean the right dose, at the right time, with the right difficulty step.
- Notifications should be state-based, not schedule-based. Trigger nudges when behavior drifts (missed sessions, worsening pain trend), not at 7pm forever. Otherwise you train users to ignore you.
- Celebrate clinically meaningful wins. Milestones tied to function (“walked stairs with less pain”) land better than streaks. Keep social features optional—rehab is private for a lot of people.
Clinical Workflow Integration
Clinicians don’t adopt apps; workflows do.
- Make the therapist view faster than the EHR. One-screen answers: who’s off-plan, who’s regressing, who needs a tweak.
- Automate the boring parts. Draft visit notes, pre-fill progress summaries, and generate a clean “what changed since last week” snapshot.
- Design for asynchronous care. Most high-leverage interventions are quick: adjust dosage, swap an exercise, send one clarifying message. If the app forces a synchronous visit for everything, it won’t scale.
Evidence-Based Exercise Protocols
This is where trust is earned—quietly.
- Build protocols as modular templates with explicit progression rules and contraindications, not as a flat list of videos.
- Version protocols like software. When you change progression logic, you should be able to answer: who was on the old version, who moved to the new one, and why.
- Outcome tracking must align with the protocol. If your protocol claims ROM improvement, your measures better reflect ROM—not just “sessions completed.”
Continuous Improvement Through Data
“Analytics” isn’t dashboards. It’s a closed loop between product, clinicians, and outcomes.
- Treat adherence as a funnel: assignment → start → completion → progression. Find where users drop and fix that step first.
- A/B test only what’s safe to vary: onboarding flow, reminder timing, explanation clarity, UI friction. Don’t experiment with clinical progression like it’s button color.
- Combine user behavior with clinician feedback: the best insights come from mismatches (patients say “too hard,” clinicians say “too easy,” completion rates tank). That’s your next iteration roadmap.
Case Studies and Success Stories
When rehabilitation app development goes sideways, it’s usually for one of three reasons: patients don’t stick with the plan, therapists can’t scale follow-ups, or “objective progress” turns out to be subjective after all. These projects show how we’ve tackled each failure mode in the real world.
Allheartz: Remote Physiotherapy and Sports Care
Allheartz built an at-home exam flow where patients record guided movements and the system extracts goniometric data from video (range-of-motion style signals) and pushes it into a clinician workflow.
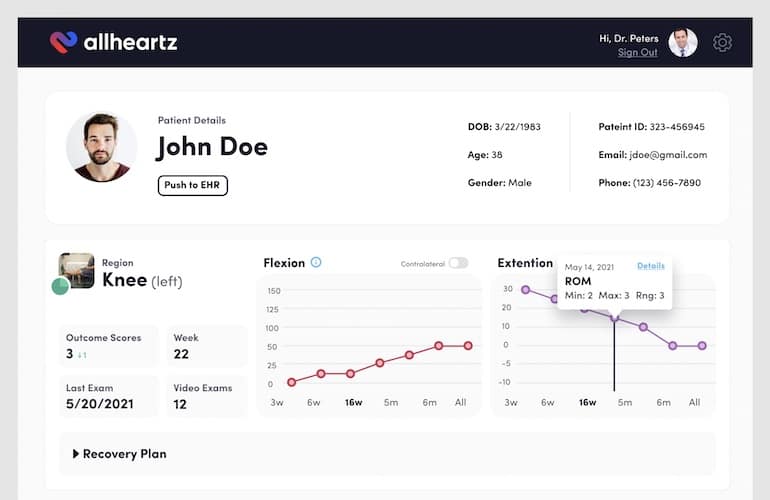
The platform pairs a patient app with a physician web dashboard (templates, progress review, video markup, and even EHR and payments hooks).
Reported outcomes include up to 50% fewer in-person visits and up to 80% less clerical time—exactly the kind of leverage clinics need to scale without burning out staff.
SoberBuddy: Behavioral Recovery and Adherence Mechanics
SoberBuddy is a CBT-based recovery app where “adherence” is daily behavior, not movement form.
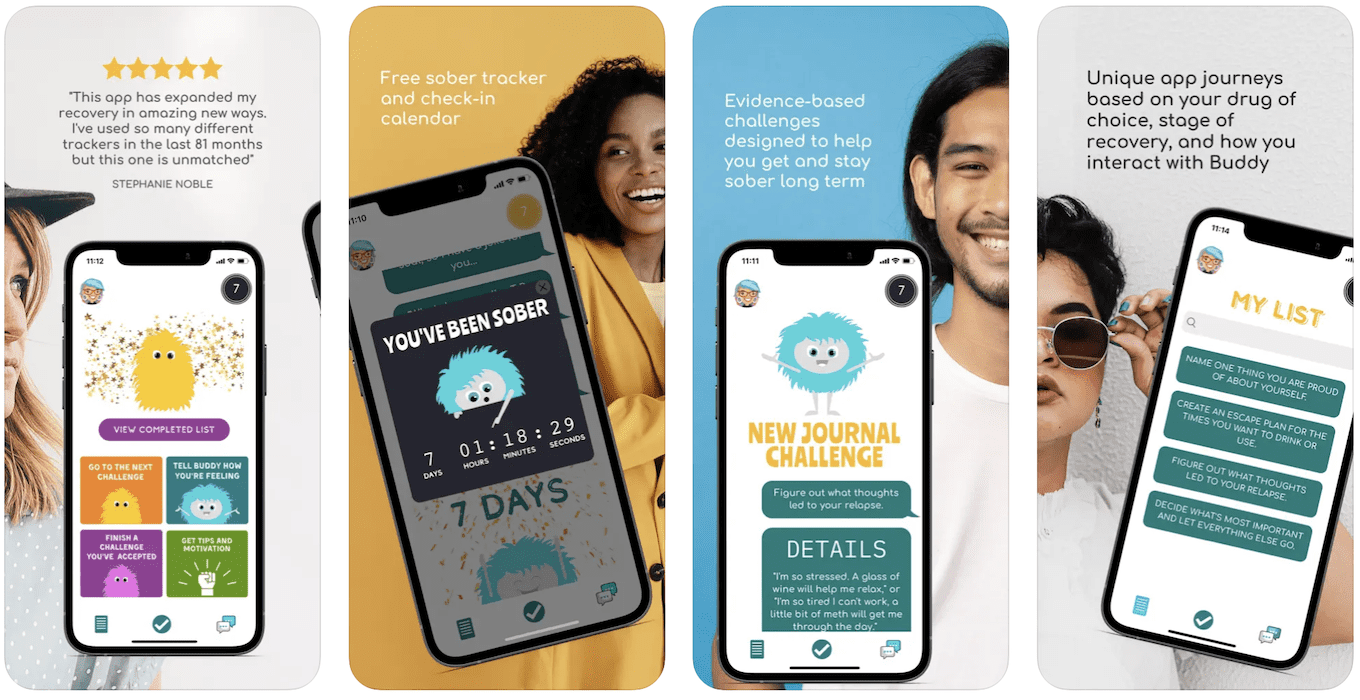
We rebuilt the product experience to keep users showing up, reporting a 300% retention lift and 40% higher engagement time alongside growth to 30,000 users—useful patterns for any rehab program that depends on consistent follow-through.
Dedica Health: Remote Patient Monitoring
Dedica is a remote monitoring platform built for a cardiology practice to replace spreadsheets and reduce manual follow-ups while staying aligned with Medicare RPM/CPT workflows.
On the clinician side, it delivers a role-based dashboard for vitals review, messaging, patient notes/medications, smart sorting, and—crucially—time tracking and billing-ready reports.
On the patient side, onboarding was simplified by avoiding a mobile app initially: patients use certified home sensors and respond to text messages, which improved adoption for the target demographic.
Reported MVP outcomes: 1,100+ patients monitored daily, a $300k/year SaaS customer, and >80% of patients reaching CPT code targets, with the business turning ROI-positive within months.
Walker Tracker: Wellness and Step Tracking at Scale
Walker Tracker shows what it takes to keep tracking systems trustworthy and motivating over time. With integrations across Apple Health/Google Fit/Samsung Health and a disciplined measurement approach (A/B tests, rollout controls), the app moved from a ~2-star rating to 4.6, while supporting 316+ billion steps across 73,000 teams. In rehab terms: fix sync issues, make progress visible, and engineer the moments that drive follow-through.
We’ve also done connected-device work (e.g., BLE-heavy builds like Joovv) when rehab products require hardware-grade reliability—useful when wearables or therapy peripherals enter the picture.
Future Trends in Digital Rehabilitation
The next wave of digital rehabilitation solutions is less “more features,” more “tighter feedback loops”: measure better, adapt faster, waste fewer clinician minutes.
VR/AR Moves From Novelty to Targeted Utility
VR has credible evidence as a pain-management adjunct (esp. chronic pain contexts). AR/MR is the longer play: guiding movement in real environments (stairs, kitchen, workplace) instead of a clinic-like sandbox—useful, but still limited by hardware fit and workflow realities.
AI Shifts From “Magic” to Auditability
The practical AI in healthcare wins are:
- predicting who will drop off
- adjusting progression rules
- flagging stalled recovery early
The differentiator won’t be model accuracy alone—it’ll be change control, transparency, and integration into clinician workflow.
Digital Biomarkers Make Rehab Continuous
Wearables + sensor data increasingly support real-world mobility tracking (gait, activity patterns) as digital biomarkers—meaning rehab decisions can be driven by what happens at home, not what looks okay during a 15-minute session.
Social Rehab Becomes “Structured Support,” Not Social Media
The useful version is small cohorts, milestones, and privacy-first accountability. The useless version is a feed.
How Topflight Can Help Build a Rehab App?
Topflight is a team of healthcare app developers who’ve shipped products where adherence, clinician workflow, and measurable outcomes actually matter—not just “nice UX.” If you’re building in rehab, we don’t start with a feature wishlist. We start with the clinical loop and the business constraints around it.
What you get when we’re the build partner:
- Scope that protects outcomes: we map your MVP to the few signals that prove value (adherence, functional progress, therapist time saved) and cut everything that’s decorative.
- Clinician-grade workflows: dashboards built for triage (“who needs attention today?”), plan adjustments, and clean documentation artifacts.
- Integration realism: we plan for the ugly parts—identity matching, data mapping, retries, audit trails, and vendor governance—so integrations don’t become your next rewrite.
- Measurement you can defend: whether you’re tracking ROM, pain trends, or sensor signals, we build a data model that’s consistent, explainable, and easy to validate.
Want to move fast without shipping a rehab-flavored fitness app? Bring us your target condition, who delivers care (PT/OT/speech), and how progress will be measured. We’ll help you choose the right lane—tracking MVP, telerehab suite, or sensing-heavy product—and define the one thing you must prove in the first 90 days. Then we build toward that proof. That’s how rehab app development stays outcome-led instead of feature-led.
Frequently Asked Questions
How much does it cost to develop a rehabilitation app?
Most MVPs land in the low-to-mid six figures if you include a therapist dashboard and HIPAA-grade basics. Costs climb quickly with video visits, EHR connectivity, billing workflows, wearables, and especially motion-analysis features.
What are the key features every rehabilitation app should have?
A structured exercise library with clear demos, simple progress tracking, therapist-facing plan creation and review, messaging/check-ins, and outcome measures that reflect the protocol. Everything else is optional until these work.
How long does it take to develop a rehabilitation app?
A solid MVP is typically 4–7 months end-to-end when you include discovery, design, build, and validation. Advanced sensing/AI, major integrations, and clinical validation can extend timelines significantly.
Do rehabilitation apps require FDA approval?
Not always. It depends on what you claim and what the app does. If it functions like clinical decision support or delivers therapeutic recommendations that clinicians rely on, you may be in SaMD territory; if it’s positioned as general wellness/education without diagnostic or treatment decision claims, it often isn’t.
What technologies are used for motion tracking in rehab apps?
Camera-based pose estimation (computer vision) is common for low-friction setups. Wearables and sensors like IMUs (accelerometer/gyroscope) add reliability when the camera can’t, and hybrid approaches fuse both.
How do rehabilitation apps ensure HIPAA compliance?
By limiting PHI exposure, enforcing role-based access, encrypting data in transit and at rest, logging access and changes, and managing vendors under BAAs where required. Operational controls matter as much as code: incident response, least privilege, retention, and audit readiness.
What's the typical ROI for healthcare organizations using rehabiliation apps?
ROI usually comes from higher adherence, fewer preventable follow-ups/readmissions, and clinician time saved through asynchronous monitoring and better triage. The exact payback depends on staffing costs, patient volume, billing model, and how well the app is integrated into workflow.