
AI-powered practice management for one specialty is different work from bolting an AI layer onto a generic system, and the gap shows up fast.
Automated prior auth that works for primary care falls apart on a fertility IVF cycle, because the clinical justification doesn’t look anything like a primary-care PA letter. Ambient documentation tuned to general psychiatry produces broken notes for medication management visits, where the template the insurance audit expects looks nothing like the one for a therapy session. A no-show model trained on family medicine scheduling data has near-zero predictive validity for pain management procedures.
The practice management software market is over $15B globally, and the specialty segment is the fastest-growing and most underserved slice of it.
So let’s separate useful practice management AI features from demo candy: which ones save time, which ones create regulatory risk, and which specialty workflows need custom architecture from day one.
How do you build a specialty PM platform with AI?
Build four Tier 1 AI modules: ambient documentation against specialty note templates, AI prior authorization letter generation, no-show prediction, and AI coding assistance with modifier logic. All four stay non-device under the January 2026 FDA CDS guidance when designed with mandatory physician review. Build them for one specialty.
Key takeaways
- AI-powered specialty practice management is a specialty data model, a specialty billing engine, and an AI pipeline built for one clinical discipline. Generic AI layered onto generic PM systems misses the specialty’s CPT and ICD-10 patterns, PA documentation requirements, outcome instruments, and compliance obligations. The AI has to be calibrated to those differences from the start.
- Depth wins over breadth. A correctly-structured mental health therapy note generated by ambient AI beats a plausible-looking generic note that fails the insurance audit. The platforms that win this market in 2026 are investing in specialty depth over AI feature count.
- Build the four safe, high-value features first. Ambient documentation, PA automation, no-show prediction, and AI coding assistance are all non-device under the January 2026 FDA CDS guidance update when designed with mandatory physician review. They have the highest ROI and the lowest FDA classification risk. Start there. Build them for one specialty. Build them well.
Table of contents
- The three tiers of practice management AI features
- Five specialties, five different builds
- The four AI healthcare practice management modules worth building first
- Generic data models break specialty practice management software in five places
- FDA classification for AI features in practice management
- 42 CFR Part 2, CLIA, and PDMP: The compliance layers HIPAA doesn’t cover
- Why choose Topflight for specialty practice management software development with AI
The three tiers of practice management AI features
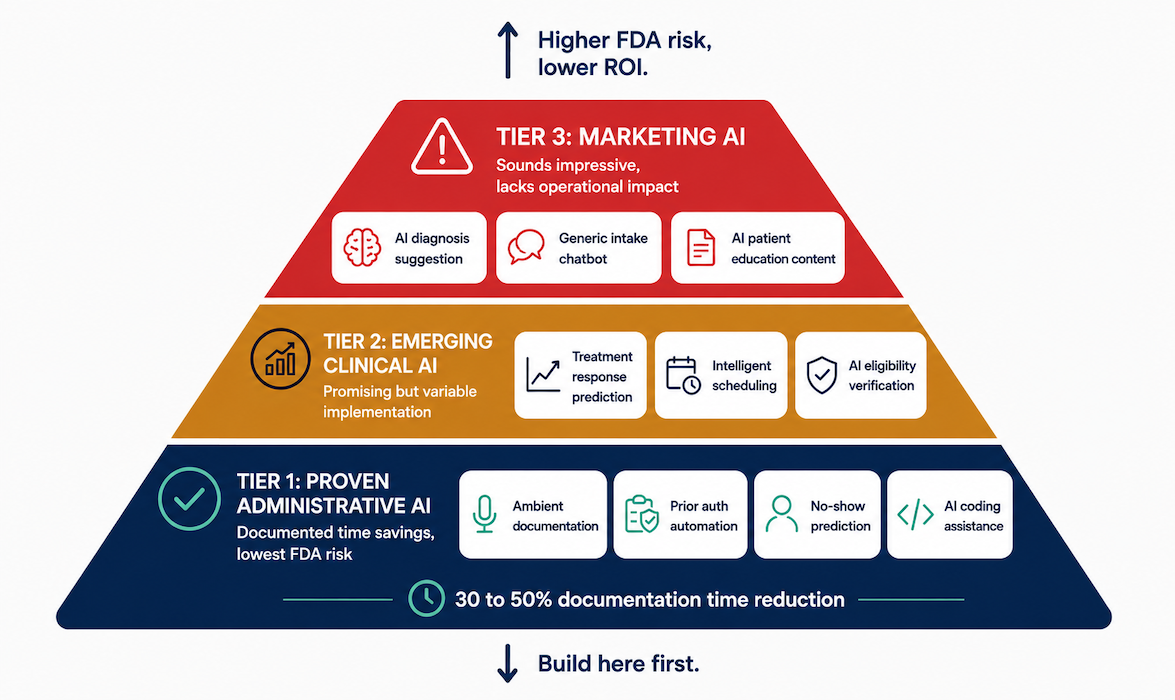
Not every AI feature deserves engineering time. The safest way to prioritize AI features is simple: ship Tier 1, treat Tier 2 as conditional, and skip Tier 3 entirely.
Generative AI in healthcare is a wide field; the practice management slice is where the bottom tier already has RCT-grade evidence and the top tier still carries FDA classification risk that catches teams at the SaMD line.
For healthcare app development in specialty markets, the ordering separates daily clinical use from demo-day abandonment.
Tier 1: AI features with documented administrative time savings
Tier 1 features have evidence of administrative time savings in deployed systems. These are the four to ship first:
Ambient AI documentation
The workflow is straightforward: capture the visit audio, transcribe it with medical ASR, generate a specialty-specific note, and route everything through a physician review queue.
The big late-2025 RCTs show time-in-note dropping 20-40 seconds per visit; Yale tracked burnout falling from 52% to 39% over 30 days. Hallucination still sits around 7% across vendors, with physical exam documentation the worst offender.
Vendor field for general use: Abridge, DAX Copilot, Nabla, Suki, DeepScribe, Ambience, Heidi Health, Commure, Freed, all running on large language model (LLM) APIs like GPT-4 and Claude API plus medical ASR with HIPAA business associate agreements (BAAs).
Eleos Health is the specialty-built AI medical scribe for behavioral health: 200+ orgs, around 70% documentation-time savings.
AI-assisted prior authorization
Structured clinical data feeds an LLM that drafts the clinical justification letter; physician reviews and signs; submission goes through Availity or CoverMyMeds.
Highest fertility billing ROI: an IVF PA letter takes 90 to 120 minutes manually, and a physician-reviewable AI draft lands in around 60 seconds.
No-show prediction
Machine learning classification on scheduling data flags high-risk appointments, triggers confirmation outreach, and overbooks at the upper threshold. The features that actually predict:
- Appointment type
- Lead time
- Patient demographics
- Prior no-show history
- Insurance type
15-25% reduction in no-show rate documented in deployed specialty scheduling AI.
AI coding assistant
Natural language processing (NLP) extracts billable services from clinical notes; a specialty code library maps to ICD-10 and CPT codes; modifier logic catches modifier 25 and modifier 59 errors before claim submission.
Biggest impact in pain management billing (E/M plus procedure codes plus modifier 25) and mental health CPT codes (E/M plus 90833 therapy add-on); this is where revenue cycle AI earns its keep in specialty practice.
Tier 2: AI features with clinical promise and variable implementation quality
Tier 2 covers features with real clinical or operational promise where implementation quality is inconsistent. Three categories worth scoping but not shipping in the MVP:
Treatment response prediction
Treatment response prediction (ML models matching patients to antidepressants or therapy modalities they’re likely to respond to) is most developed in mental health, but the training data bar is high. Most single-specialty practices don’t have the patient volume for a reliable practice-specific model.
Intelligent scheduling optimization
Predictive scheduling optimization allocates slots across appointment types and providers to maximize utilization and revenue per provider hour. High value for fertility, where embryologist time and procedure suite capacity are hard constraints. Moderate value for mental health.
AI-powered eligibility verification
AI-powered eligibility verification (NLP extraction of specialty benefit details from payer responses) earns its slot in specialties with complex benefits:
- fertility cycle benefits
- mental health parity verification
- pain prior-auth thresholds
- sleep DME approvals
Tier 3: marketing AI features that sound impressive but lack operational impact
Tier 3 features sound impressive in demo and don’t move the needle in practice. Generic patient intake chatbots lose to structured forms on error rate and friction, especially for non-English speakers and older patients; specialty intake needs PHQ-9 or fertility history, which a chatbot doesn’t administer reliably. AI-generated patient education sounds useful until physician review burden swallows the time savings.
The dangerous one is AI diagnosis or treatment recommendation shipped without close physician oversight. A mental health AI suggesting a DSM-5 diagnosis from intake data, or a fertility AI proposing a stimulation protocol, is acting as clinical decision support at minimum and probably as SaMD. FDA classification gets hairy fast. Patient safety gets hairier.
When a generic platform is actually the right call
A generic platform is sometimes the right call for AI medical practice management work, and pretending otherwise wastes everybody’s time. Pre-product-market-fit MVPs, solo practices without the volume for a specialty buildout, multi-specialty groups where depth-per-specialty is shallow. Generic platforms ship adequate scheduling and billing today, with basic AI built in:
- Athenahealth
- eClinicalWorks
- AdvancedMD
- DrChrono
The line to watch: when specialty depth becomes the bottleneck on billing accuracy, PA time, or documentation fit, the generic platform’s AI roadmap won’t catch up in time. That’s the trigger for the custom build.
Five specialties, five different builds
One size fits none in specialty PM. Mental health practice management software, fertility EHR, pain management EHR, sleep medicine software, and functional medicine practice management all look similar on paper, then immediately diverge in billing, documentation, compliance, and AI ROI.
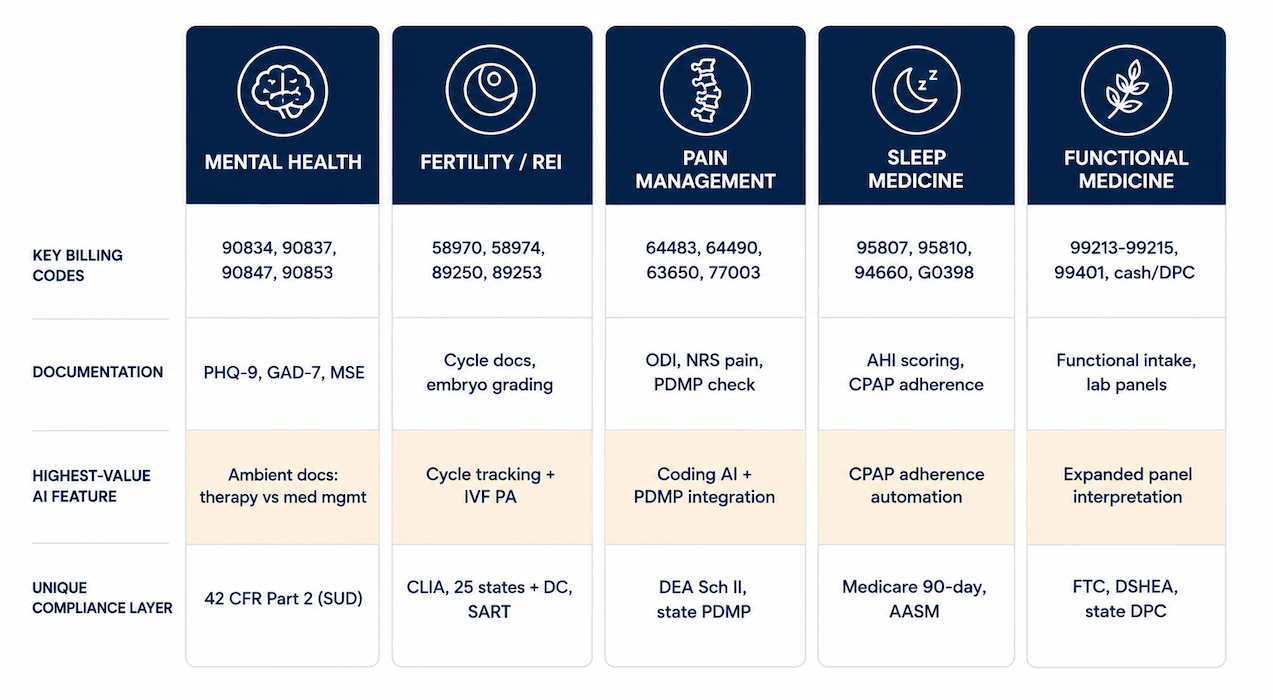
Each has a different billing code set, specialty-specific documentation pattern, highest-impact AI feature, and compliance layer that HIPAA does not cover. They share the same plumbing:
- referral management
- telehealth integration
- scheduling
- intake.
Picking one before you architect anything is the first real decision in any specialty EHR with AI build.
| Specialty | Billing codes | Specialty documentation | Highest-impact AI feature | Compliance hook |
| Mental health | 90834, 90837, 90847, 90853 (therapy and group); 99213-99215 + 90833 for med management; H0015 and H2019 for Medicaid IOP/PHP | PHQ-9 and GAD-7 outcome measurement, Columbia SSRS; therapy notes with modality; med-management with mental status exam; session-type distinction | Ambient documentation with therapy vs med-management template split; PHQ-9 and GAD-7 auto-scoring with episode-level trend | 42 CFR Part 2 for SUD treatment; mental health parity verification; confidentiality restrictions beyond standard HIPAA |
| Fertility / REI | IVF billing codes 58970, 58974, 89250, 89253; S4981-S4993 cycle-specific Medicaid codes; Z31.x diagnosis | Cycle documentation (stimulation, monitoring, retrieval, transfer); embryo grading and selection; cryopreservation records; genetic testing; cycle outcomes | Cycle tracking dashboard with AI outcome prediction; employer benefit integration (Carrot, Progyny); IVF PA automation | CLIA for embryology lab; 25 states plus DC now mandate IVF insurance coverage (up from 19 post California SB 729); embryo disposition consent; SART CORS submission |
| Pain management | 64483, 64490, 62321, 63650; E/M with procedure (modifier 25); fluoroscopy 77003 and 77012 | ODI functional outcomes, NRS pain, opioid risk tool (ORT); PDMP check documentation; interventional procedure notes with fluoroscopy findings | AI coding for E/M + procedure + modifier 25 logic; PDMP integration with automated check; PA automation for SCS and intrathecal pump | DEA Schedule II prescribing; specialty formulary restrictions on long-acting opioids; state PDMP mandates; CDC opioid guideline (2022 update) |
| Sleep medicine | 95807, 95808, 95810 for in-lab PSG; 94660 (CPAP initiation); G0398-G0400 for home sleep testing; DME billing for CPAP/BiPAP | Sleep study interpretation; AHI scoring; CPAP adherence (4+ hours/night for 21 of 30 days for Medicare); HST vs in-lab decision docs | Automated CPAP adherence ingestion from device feeds (ResMed AirView, Philips EncoreAnywhere); AI-drafted PSG reports; PA automation for HST vs in-lab | CPAP DME billing separate from professional services; 90-day Medicare compliance documentation; AASM accreditation |
| Functional / integrative | 99213-99215; 99401-99404; cash-pay and DPC models; membership billing; supplement dispensing outside insurance | Functional intake (symptom timeline, toxin exposure, dietary); expanded lab panel interpretation; supplement and lifestyle protocols | AI lab interpretation for expanded panels (organic acids, DUTCH hormone, micronutrient); membership engagement AI; cash-pay estimate automation | FTC functional medicine claim guidelines; state scope of practice for non-MD; DSHEA; state DPC agreement compliance |
Pain management and sleep medicine sit closest to general chronic disease management app work; the others are more disjoint. Market signal is strongest in mental health: 160M+ Americans live in professional shortage areas for mental health care, and 93% of behavioral health workers experience burnout (National Council for Mental Wellbeing).
That workforce reality alone explains why mental health is the highest-volume specialty PM segment in 2026.
The four AI healthcare practice management modules worth building first
If you’re building for a specialty practice, start with the four AI modules that already have evidence, workflow fit, and regulatory breathing room:
- ambient documentation
- prior authorization automation
- no-show prediction
- coding assistance
Each one has a defined architecture, named buy/build trade-offs, and a specialty-depth requirement that determines whether the deployed system gets daily clinical use. AI healthcare practice management work that skips specialty depth fails the audit.
These four are also the four with the clearest FDA classification: non-device under the 2026 CDS framework when the physician review gate is wired in correctly.
Module 1: Ambient AI documentation for specialty notes
Ambient AI documentation is a six-stage pipeline: audio capture, medical ASR, speaker diarization, clinical entity extraction, specialty-template note generation, and a physician review queue that decides whether the system survives deployment.
Buy medical ASR (Deepgram, AssemblyAI, AWS Transcribe Medical, Microsoft Speech) and LLM APIs (GPT-4/5, Claude via Bedrock, Gemini, Azure OpenAI), all with HIPAA BAAs. The ChatGPT HIPAA compliance story has matured: every major LLM provider now signs BAAs for healthcare with subprocessor disclosures that hold up in an audit.
Build the specialty prompt layer and the physician review queue yourself. HIPAA compliant app development for ambient documentation centers on the LLM-output review architecture and the audit log of physician edits.

AI clinical documentation specialty products live or die on template fit. The templates that matter, per discipline:
- Mental health: therapy SOAP with modality; med-management with mental status exam; crisis docs using the Columbia protocol; group session notes with composition and participation
- Fertility: consultation (history, diagnosis, treatment options); cycle monitoring; procedure notes; embryology lab notes
- Pain: interventional procedure notes with fluoroscopy findings; med-management with PDMP review; ODI and NRS functional assessment
- Sleep: PSG interpretation (AHI, sleep architecture, desaturation, PAP titration); CPAP follow-up with adherence and pressure optimization
Builder Alert: A mental health scribe that uses pain-management vocabulary, or skips mandatory session-modality documentation required for insurance billing, creates more work than it saves.
Module 2: AI prior authorization automation
Prior authorization is where specialty depth pays for itself quickly. The workflow usually breaks into four parts:
- Payer requirement library: procedure → required justification elements; refines over deployment from payer portals and prior PAs.
- Clinical data extraction: diagnosis codes, functional scores, and treatment history pulled into payer format.
- LLM letter generation: clinical justification against payer- and specialty-specific templates.
- Physician review and submission: Availity, CoverMyMeds, or specialty platforms (Cohere Health, Rhyme).
The CMS Interoperability and Prior Authorization Final Rule (January 2024) requires certain payers to implement Prior Authorization Requirements, Documentation, and Decision (PARDD) APIs and Patient Access APIs by January 2027. The integration target moves as PARDD rolls out; design the submission layer to flex with it.
Clearinghouse integration on the back end wires PA into the broader revenue cycle management workflow: EDI 837 for claims, real-time eligibility for insurance verification, and eligibility checking against payer-specific benefit structures.
Module 3: No-show prediction and scheduling intelligence
No-show prediction is the least mysterious ML build in this stack, which is good news because appointment scheduling AI needs clean historical scheduling data.
Training data bar: 10,000 historical scheduled appointments with no-show outcome labels. Below that, use a pre-trained no-show management model from LeanTaaS, Experian Health, Relatient, or Notable.
Specialty features carry the signal: pain procedure appointments behave differently from pain E/M; fertility monitoring approaches zero no-show because patients are motivated; mental health has the highest no-show rates in any specialty, at 15-30%.
Gradient boosting (XGBoost, LightGBM) outperforms logistic regression and neural networks on tabular scheduling data at typical practice volumes. Deep learning earns its slot at 100K+ appointment training sets.
Intervention thresholds:
- >40% no-show probability triggers patient engagement via automated appointment reminders and confirmation outreach
- >70% triggers overbooking logic or waitlist management fills
Calibrate against your no-show cost and overbooking tolerance, then feed the prediction score into downstream scheduling optimization for recall management and care coordination after no-show events.
Module 4: AI coding assistance
AI coding assistance, the engine behind AI medical billing in specialty practices, has high adoption where coding complexity and revenue impact are both high.
Pipeline:
- NLP extracts billable services and diagnoses from clinical notes
- specialty code library maps to CPT and ICD-10
- modifier logic catches modifier 25, modifier 59, and 26/TC errors
- physician or biller review gate before claim submission
Named platforms: Suki (ICD-10/HCC suggestion baked into the scribe), Ambience (coding plus clinical documentation integrity), DeepScribe (E/M coding focus), 3M M*Modal CDI Engage.
The Cigna trap, October 2025: Cigna started auto-downcoding Level 4-5 E/M claims by one level unless the documentation clearly supports the higher complexity. Aetna Better Health rolled out similar reviews soon after. Ambient scribe vendors spent 2024 and 2025 pitching richer documentation as the revenue play. The payers are clawing it back, and revenue cycle management AI is no longer a one-sided arms race.
Builder Alert: AI coding without physician review is False Claims Act exposure. Upcoding a 99214 to 99215 and submitting without review is fraud regardless of intent. The audit log of accepted, modified, and rejected AI suggestions is the practice’s CMS audit defense. Build the review gate as a hard requirement.
Generic data models break specialty practice management software in five places
Generic practice management data models fail for specialty healthcare in five predictable places. AI in EHR features amplify these failures: an ambient scribe writing to an encounter-centric data model can’t aggregate cycle-level fertility outcomes, no matter how clean the note generation is.
A specialty PM platform, whether single-tenant or multi-tenant SaaS on cloud infrastructure, has to be built around the right object model from the start.
Encounter-centric vs episode-centric data models
Generic PM organizes data around encounters. Specialty care often organizes around episodes. IVF cycle management is the cleanest example: 12-20 monitoring appointments, retrieval, embryo transfer, and follow-up, all linked to a single cycle with cycle-level outcomes (live birth rate, embryo count, cumulative success). A pain SCS implantation is an episode comprising a trial period and permanent implant, with follow-up programming visits anchored to the same record.
The data model has to support episode-level aggregation, and how to integrate with Epic EHR for episode patterns is where most teams burn a quarter on FHIR R4 Encounter mismatches. The EHR integration choice cascades into every downstream module.
Device and equipment tracking
Sleep medicine, orthotics/prosthetics, and some pain practices dispense or prescribe durable medical equipment.
For sleep medicine, orthotics, prosthetics, and some pain workflows, device dispensing records need to connect back to encounters, claims, compliance documentation, and adherence feeds.
None of this fits the standard FHIR R4 patient-encounter-observation triangle without custom resources.
Outcome instrument scoring and trending
Specialty outcomes get measured with validated instruments:
- PHQ-9
- GAD-7
- ODI
- AHI
- Columbia Suicide Severity Rating Scale
Instrument scores need indexing by administration date and treatment episode, so trending across episodes works off the index. Generic problem-list-centric data models can’t do this. The Epic Flowsheet pattern handles it as a backstop.
Behavioral health software and other specialty platforms build dedicated instrument-and-score schemas from day one.
Multi-provider care team coordination
Fertility care involves REI physicians, nurses, embryologists, genetic counselors, and mental health consultants. Pain involves interventional physicians, PTs, and addiction medicine consultants.
Care-team coordination also needs first-class roles, task ownership, documentation responsibility, and episode-level handoff audit trails. API-first design over older HL7 v2 messaging is the architectural shift; the Epic Care Team resource is a starting point that specialty platforms extend with role-specific permissions.
Specialty-specific consent management
Fertility cycle-specific consents are unique: embryo disposition, genetic testing (PGT-A/M) consent, donor gamete consent if applicable, and cryopreservation duration agreements. SUD treatment under 42 CFR Part 2 needs patient-specific consent for record sharing on top of standard HIPAA TPO authorization.
Pain management needs informed consent for interventional procedures and controlled substance agreements. Generic consent management modules accommodate none of these without custom workflow extensions.
FDA classification for AI features in practice management
FDA classification hinges on what the AI does with clinical information and whether a clinician can independently review the basis of its output. The FDA clinical decision support (CDS) exemption under the 21st Century Cures Act decides which features stay non-device and which cross into SaMD.
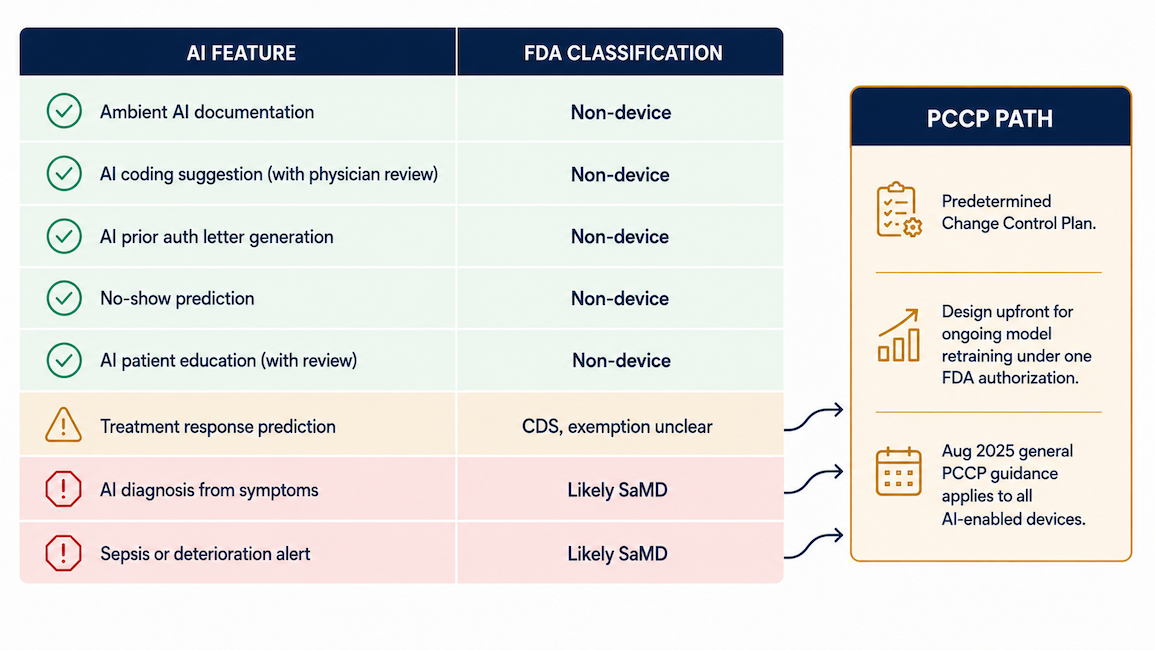
The picture is mid-shift in 2026, and AI in healthcare compliance work has to track both the January FDA CDS guidance update and the PCCP path.
| AI feature | FDA classification | Rationale and builder requirement |
| Ambient AI documentation | Non-device | Documents physician decisions before EHR write. Mandatory review gate plus audit trail of AI suggestion vs physician-approved final. |
| AI coding suggestion | Non-device (if reviewed) | Administrative coding function; physician or biller reviews suggestion. Log accepted vs modified vs rejected. |
| AI PA letter generation | Non-device | Administrative documentation; physician reviews and signs before submission. Log AI-generated vs physician-edited content. |
| No-show prediction | Non-device | Administrative scheduling function. Label predictions as scheduling tools; do not link to clinical triage or care prioritization. |
| AI-generated patient education | Non-device (if reviewed) | Administrative patient communication; physician reviews content before distribution. |
| Treatment response prediction | CDS, may not be exempt | Recommendation affecting treatment selection. FDA classification assessment required; 510(k) likely. |
| AI diagnosis suggestion | Likely SaMD | Clinical decision affecting patient management. Do not build without 510(k) clearance. |
| Sepsis or deterioration alert | Likely SaMD | Time-sensitive CDS with patient harm potential from false negatives. Not appropriate for ambulatory specialty PM without clearance. |
Builder Alert: The CDS exemption requires that the clinician “can independently review the basis for the recommendations.” That’s a design requirement. A black-box model whose recommendations can’t be traced back to specific clinical data points fails the test regardless of the review workflow. Explainability is the substrate of the exemption.
That means explainability is not a nice-to-have UX layer. If the recommendation cannot be traced back to specific clinical data points, the review workflow alone will not save it.
What the January 2026 FDA CDS guidance update changes
The FDA CDS final guidance published January 6, 2026 supersedes the 2022 version and broadens the agency’s interpretation of Criterion 3. FDA will ease enforcement on certain CDS software that recommends a single diagnosis or treatment to a healthcare provider, where the prior reading was stricter.
The shift reflects the Trump administration’s AI deregulation push: the January 2025 EO “Removing Barriers to American Leadership in AI” and the July 2025 AI Action Plan.
Caveat per Arnold & Porter and ACR analyses: the 2026 update doesn’t expressly change FDA’s AI approach. Commissioner Makary stated further deregulation and a risk-based AI framework are forthcoming. Plan around what’s on paper today.
PCCP: the new path for AI features that do require clearance
PCCP, the Predetermined Change Control Plan, is the mechanism that handles model retraining for AI features that need FDA clearance. Statutory basis: Section 515C FD&C Act, added by FDORA in December 2022. AI/ML-specific PCCP guidance landed December 2024; general PCCP guidance covering all AI-enabled devices was finalized August 2025.
Three components:
- description of modifications
- modification protocol
- impact assessment
Once authorized, modifications inside scope deploy without new submissions. Outside-scope changes still need new submissions; intended use can’t change.
For a treatment response prediction model on the health AI FDA clearance path, a PCCP makes ongoing retraining viable. Without one, every meaningful model update is a new submission.

What’s still unsettled in 2026
Three things keep the 2026 FDA AI picture genuinely unsettled. Loper Bright v Raimondo (June 2024) overturned Chevron deference, leaving the FDA’s interpretive choices in CDS guidance, PCCP scope, and SaMD classification legally vulnerable. The Trump administration’s deregulation push moves the same direction. FDA itself has signaled more changes are coming.
Honest move: build clearly non-device features (the Tier 1 four) without PCCP. Design borderline features with explainability built in and a PCCP-ready architecture. That keeps your options open whichever way the regulation goes.
42 CFR Part 2, CLIA, and PDMP: The compliance layers HIPAA doesn’t cover.
The HIPAA Security Rule is the floor for healthcare PHI handling. Three specialty compliance layers sit on top of it, each with its own audit trail, role-based access control, and SOC 2 Type II implications. HIPAA compliant software development gets you ready for the BAA; what follows is what comes after.
42 CFR Part 2: enforcement is live as of February 16, 2026
OCR began civil enforcement of 42 CFR Part 2 (substance use disorder confidentiality) on February 16, 2026, after announcing the Part 2 noncompliance enforcement priority on February 13. The Final Rule itself took effect April 16, 2024, implementing CARES Act Section 3221 to align Part 2 with HIPAA.
What the system has to do:
- Flag SUD treatment records with Part 2 status in the data model
- Require patient-specific consent for Part 2 record disclosure through the patient portal, care summary exports, and EHR integration, even where a broad HIPAA TPO authorization is in place
- Track Part 2 record access separately in the audit log
The 2024 rule changes have concrete system implications:
- Single TPO consent now covers all future TPO uses and disclosures, replacing per-disclosure consents
- HIPAA-regulated entities receiving Part 2 records under valid TPO consent may redisclose per HIPAA, except for civil, criminal, administrative, or legislative proceedings against the patient (separate consent or court order required)
- HIPAA Breach Notification Rule now applies to Part 2 breaches
- SUD counseling notes get psychotherapy-note-style protection: separate consent required, no blanket TPO release
- Notice of Privacy Practices update is required, combinable into a single HIPAA-plus-Part-2 document
- Physical segregation of Part 2 records is no longer required
CLIA and fertility lab compliance
CLIA is the federal program administered by CMS that oversees clinical lab testing on humans. Fertility embryology labs run under high-complexity CLIA certification.
System support areas: test reporting, instrument quality control, personnel qualifications, and proficiency testing records. SART CORS (Clinic Outcome Reporting System) annual cycle outcome submission is required for SART membership and CDC reporting; the system has to extract cycle-level data and format it for SART.
The No Surprises Act adds another layer of fertility clinic compliance where the clinic offers cash-pay alongside insurance.
PDMP integration for pain management
All 50 states and DC operate PDMPs. The integration layer that matters: PMP InterConnect (NABP-operated) for interstate sharing, and PMP Gateway or Narxcare (Bamboo Health, formerly Appriss Health) for in-EHR queries from within the clinical workflow.
State mandates vary on timing: some require a check before every Schedule II-V prescription, some only before opioids, some initial-plus-every-3-months for long-term opioid therapy.
The CDC opioid prescribing guideline (2022 update) is the documentation baseline. The system checks the PDMP, logs the check, links the result to the prescribing event, and surfaces the Narxcare risk score in the prescribing UI.
Build vs buy your AI practice management software, feature by feature
AI practice management software is a stack of components. Some are commodities to buy through an API; others are the specialty depth that defines the product. Get the split right and the architecture works; get it wrong and you either reinvent the wheel or ship a shallow clone.
| Component | Build | Buy / API |
| Ambient AI documentation | Specialty note templates, entity extraction prompts, physician review queue | ASR (Deepgram, AssemblyAI, AWS Transcribe Medical, Microsoft Speech), LLM APIs (OpenAI, Anthropic, Google, Microsoft Azure OpenAI) with HIPAA BAAs |
| AI PA letter generation | Specialty PA templates, payer requirement library, denial appeal logic | LLM API with BAA; submission integration through Availity, CoverMyMeds, Cohere Health, Rhyme |
| No-show prediction | Practice-specific model when historical appointment volume exceeds 10,000 | Pre-trained scheduling AI (LeanTaaS, Experian Health, Relatient, Notable) for smaller practices |
| AI coding assistance | Specialty code library, modifier 25 / 59 / 26/TC logic, review-gate audit log | Coding AI APIs (Suki, Ambience, DeepScribe, 3M M*Modal CDI Engage) |
| Functional medicine lab interpretation | Custom interpretation for expanded panels (organic acids, DUTCH hormone, micronutrient) | LabCorp and Quest APIs for standard reference range data |
| PDMP integration | None | PMP InterConnect (NABP) for interstate, PMP Gateway or Narxcare (Bamboo Health) for in-EHR queries |
| CPAP adherence data | None | ResMed AirView API, Philips EncoreAnywhere API |
| SART CORS reporting | Cycle-level data extraction and CDC-format submission | None available |
The split that holds across every row: own the specialty depth, API the commodities.
- specialty templates
- payer requirement libraries
- episode-centric data models
- modifier logic
- expanded panel interpretation
- SART data extraction
☝ Those are the moat.
- ASR transcription
- base LLMs
- PDMP queries
- DME data feeds
- EHR integrations
☝ Those are infrastructure.
When evaluating buy options, the criteria that matter beyond raw capability: BAA terms (and whether the subprocessor list holds up to audit), pricing model fit (per-encounter vs per-provider vs flat), latency at scale, and uptime SLA.
Specialty PM products run on real-time clinical workflows; an ASR vendor with a 99.9% SLA and 800ms p95 latency is operationally different from one with 99.5% and 2s.
Healthcare app development cost trails the split as a consequence: buy the commodities and the recurring API costs scale with usage; build the depth and the upfront engineering investment compounds into product defensibility.
Why choose Topflight for specialty practice management software development with AI
Topflight builds AI-powered healthcare applications for specialty practice markets, including ambient AI documentation, prior authorization automation, and specialty-specific clinical data systems. We work at the intersection of AI architecture and specialty billing and compliance, which is where adoption happens or breaks.
What we bring to specialty PM engagements:
- Ambient AI documentation: specialty note template libraries, medical ASR integration with HIPAA BAAs, LLM prompt engineering for clinical note generation, physician review queue design
- Prior authorization AI: specialty PA letter generation, payer requirement library development, Availity and CoverMyMeds integration, denial appeal automation
- Specialty data models: episode-centric architecture, outcome instrument scoring and trending, specialty-specific consent management, care team coordination
- FDA classification guidance: AI feature regulatory risk assessment, CDS exemption architecture, explainability design for physician review, PCCP-ready architecture for borderline features
- Specialty compliance: 42 CFR Part 2 SUD record handling (now under live OCR enforcement), CLIA lab compliance documentation, PDMP integration via PMP Gateway and InterConnect, SART CORS reporting, HIPAA-compliant PHI architecture
Selected past work in adjacent AI healthcare territory: GaleAI, NLP and GenAI for medical coding; LnQ, on-demand radiology with deep EHR integration; Mi-Life, AI care navigation in mental health.
Building AI-powered practice management for a specific specialty (mental health, fertility, pain management, sleep medicine, or functional medicine) is where AI architecture and specialty depth either reinforce each other or fail in production.
If you’re scoping a product like that, talk to Topflight about your specialty billing requirements, AI feature priorities, and FDA classification path. We can help you build specialty practice management software that gets daily clinical use long after the demo.
Frequently Asked Questions
What AI features should specialty practice management software have in 2026?
Four Tier 1 features: ambient AI documentation, prior authorization automation, no-show prediction, and AI coding assistance. All four are non-device under the January 2026 FDA CDS guidance when designed with mandatory physician review.
Is AI-generated clinical documentation considered a medical device by the FDA?
No. Ambient AI documentation is non-device under the 21st Century Cures Act CDS framework, reaffirmed in the January 2026 FDA final guidance, when physician review happens before EHR write.
How does AI prior authorization automation work for specialty practices?
Four stages: payer requirement library, clinical data extraction from the patient record, LLM-generated PA letter, physician review before submission through Availity or CoverMyMeds. Highest ROI in fertility, where IVF letters drop from 90-120 minutes manual to around 60 seconds as an AI draft.
What is the difference between a general EHR and specialty practice management software?
A general EHR is encounter-centric and discipline-agnostic. Specialty PM is episode-centric and built around the specialty’s billing codes, modifier logic, outcome instruments, and compliance obligations.
Can AI coding assistance be used without physician review?
No. AI coding without physician or biller review creates False Claims Act exposure: upcoding without review is fraud regardless of intent. The audit log of accepted, modified, and rejected suggestions is the practice’s CMS audit defense.