
In the U.S., chronic disease management app development is no longer a niche health-tech bet. Chronic diseases remain the leading drivers of healthcare costs, and CDC figures still support the familiar headline: roughly 6 in 10 adults have at least one chronic disease, while 4 in 10 have two or more. More recent CDC data also shows that about 90% of the nation’s $4.9 trillion in annual healthcare spending goes to people with chronic and mental health conditions.
That is why the modern chronic disease management app has become infrastructure, not garnish: the daily layer that supports glucose control, blood pressure visibility, inhaler adherence, and longitudinal care for patients with comorbidity across settings. CMS now recognizes RPM billing through CPT 99453, 99454, 99457, and 99458, while employers are also buying condition-specific programs as part of broader employer benefits and population health strategy. Mercer reports that 32% of large employers already offer stand-alone diabetes programs.
This guide breaks down what it actually takes to build across five major conditions: device integrations, reimbursement logic, FDA risk, and the technical architecture choices that decide whether the product is useful in the wild or just another polished demo with commitment issues.
What does it take to build a chronic disease management app?
To build a chronic disease management app, you need more than a patient-facing tracker. A viable product combines condition-specific workflows, connected device data, clinician dashboards, reimbursement logic, and a compliance strategy that fits the actual risk level of the features you are shipping. In practice, the hardest decisions are not UI decisions but architecture, regulatory scope, and workflow design.
Key Takeaways
- A chronic disease management app is really two products at once: a patient experience layer and a clinical operations layer with alerting, documentation, and reimbursement support.
- The architecture changes by condition. Diabetes, hypertension, COPD, heart failure, and mental health all have different device, workflow, and FDA-risk profiles.
- The strongest CDM apps are designed around real care delivery from day one: EHR integration, RPM or CCM billing workflows, and compliance controls are not add-ons.
Table of Contents
- What Is a Chronic Disease Management App?
- The Chronic Disease App Matrix — Five Conditions, Seven Dimensions
- Diabetes Management App Development
- Hypertension Management App Development
- COPD and Asthma Management App Development
- Heart Failure Management App Development
- Mental Health and Behavioral Health App Development
- Universal Architecture for Chronic Disease Management Apps
- Reimbursement Pathways for CDM Apps — The CPT Codes That Matter
- HIPAA, FDA, and SOC 2 for CDM Apps — The Compliance Stack
- The CDM App Development Process — Phase by Phase
- Why Choose Topflight for Chronic Disease Management App Development
What Is a Chronic Disease Management App?
A chronic disease management app is a digital health platform that helps patients manage a specific chronic condition through continuous data capture, personalized guidance, communication with care teams, and integration with clinical workflows.
The strongest products do not behave like glorified symptom diaries. They operate across four functional layers that together create clinical and business value.

Layer 1 — Data Collection
This layer builds the longitudinal record. Passive inputs come from connected devices such as:
- CGMs
- blood pressure cuffs
- pulse oximeters
- smart scales
- wearables
Active inputs include:
- symptoms
- food logs
- medication adherence
- mood check-ins
- other patient-reported outcomes
The design rule here is brutal but simple: the more friction you force on the patient, the faster usage drops. Good CDM products automate what they can and ask only for what matters.
Layer 2 — Intelligence and Alerting
Raw readings become useful only when the app interprets them. This layer handles trend analysis, threshold-based alerts, and personalized recommendations. It is also where regulatory trouble begins. Depending on how alerts or recommendations are framed, features can move from general wellness into clinical decision support or FDA-regulated software.
This is also where teams start asking “How will AI help change EHR workflows rather than just decorate them?” CMS’s RPM framework also makes this layer financially relevant, because the workflow must support services tied to CPT 99457 and 99458.
Layer 3 — Patient Engagement
This is the behavior-change engine: reminders, education, coaching, progress tracking, messaging, and other mechanisms that sustain patient engagement around a care plan. Without it, the rest of the stack is a shiny machine with no fuel.
In practice, a lot of value here overlaps with conversational AI in healthcare, but the app still has to feel clinically grounded, not like a chatbot that read half a wellness blog and got overconfident.
Layer 4 — Care Team and Clinical Integration
This is the B2B layer. A clinical dashboard, care coordination, telehealth integration, and remote patient monitoring (RPM) workflow turn patient data into something a provider can actually act on. In U.S. clinical settings, that usually means FHIR-based exchange, and SMART on FHIR remains the standard launch framework for opening apps inside EHR workflows.
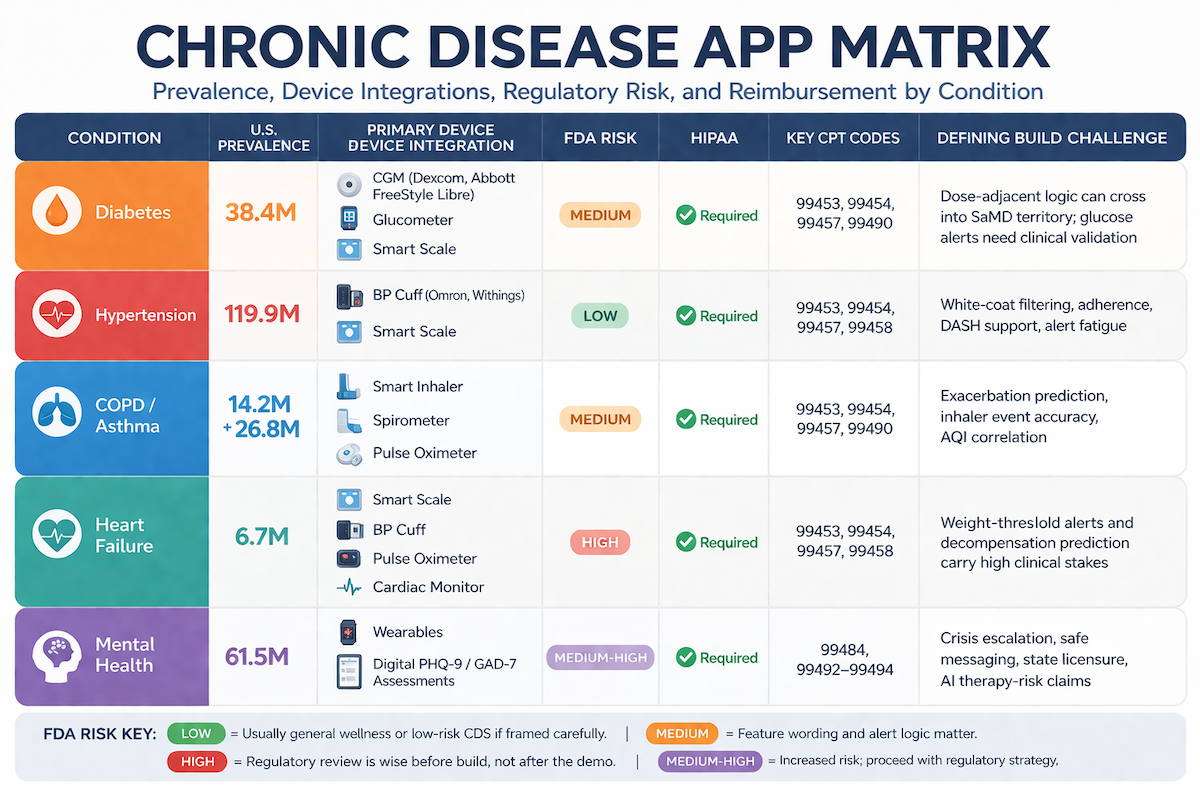
The Chronic Disease App Matrix — Five Conditions, Seven Dimensions
If you are planning companion app development for chronic care, this is the fastest way to see where the real complexity sits: not in the login screen, naturally, but in device data, reimbursement logic, and regulatory risk.
For buyers in value-based care, payer integration, and accountable care organization (ACO) settings, the matrix also shows which categories benefit most from real-time monitoring and which ones become workflow grenades if implemented casually.
| Condition | U.S. prevalence | Primary device integration | FDA risk | HIPAA | Key CPT codes | Defining build challenge |
| Diabetes | 38.4M | CGM (Dexcom, Abbott FreeStyle Libre), glucometer, smart scale | Medium | Required | 99453, 99454, 99457, 99490 | Dose-adjacent logic can cross into SaMD territory; glucose alerts need clinical validation |
| Hypertension | 119.9M | BP cuff (Omron, Withings), smart scale | Low | Required | 99453, 99454, 99457, 99458 | White-coat filtering, adherence, DASH support, alert fatigue |
| COPD / Asthma | 14.2M + 26.8M | Smart inhaler, spirometer, pulse oximeter | Medium | Required | 99453, 99454, 99457, 99490 | Exacerbation prediction, inhaler event accuracy, AQI correlation |
| Heart Failure | 6.7M | Smart scale, BP cuff, pulse oximeter, cardiac monitor | High | Required | 99453, 99454, 99457, 99458 | Weight-threshold alerts and decompensation prediction carry high clinical stakes |
| Mental Health | 61.5M | Wearables, digital PHQ-9/GAD-7 assessments | Medium-High | Required | 99484, 99492–99494 | Crisis escalation, safe messaging, state licensure, AI therapy-risk claims |
FDA risk key:
- Low = usually general wellness or low-risk CDS if framed carefully.
- Medium = feature wording and alert logic matter.
- High = regulatory review is wise before build, not after the demo impressed everyone and then legal showed up.
Diabetes Management App Development
Diabetes management app development is one of the most mature and competitive corners of digital health, which is exactly why generic wellness tracking does not cut it. The latest U.S. figures put diabetes at 38.4 million people and prediabetes at 97.6 million adults. That scale matters because diabetes is a daily management problem, not an occasional-visit problem.
What a Diabetes CDM App Must Do Differently
A serious diabetes app has to connect behavior to glucose in a way that is both clinically useful and easy to act on. That starts with the continuous glucose monitor (CGM). Manual logging gives you a few snapshots a day; CGM systems typically generate readings every 5 minutes, or about 288 readings per day, which is why they are foundational for trend detection, alerting, and tighter glycemic control.
That data only becomes useful when paired with context. Meal logging, medication adherence, insulin timing, activity, and stress all shape the pattern. In practice, the strongest products for diabetes mellitus make carb logging as painless as possible, tie insulin or medication events to glucose curves, and present trend metrics that matter to both patients and clinicians. Estimated A1c can be useful, but it must be framed as an estimate derived from glucose patterns, not a lab result.
FDA Classification for Diabetes Apps
The risk line runs straight through dosing. An app that displays glucose data and trends is one thing. An app or AI health coaching layer that tells a patient to adjust insulin is another. FDA-cleared products already exist for insulin dose calculation, which is the clearest reminder that dose-adjacent logic is not casual feature creep; it is regulated territory.
Builder alert: if your app says anything close to “consider adjusting your basal dose,” get a regulatory opinion.
Technical Architecture — Diabetes
On the integration side, Dexcom has an official developer platform, while Abbott’s Libre ecosystem is widely used through LibreView and LibreLinkUp-based data flows. In a production app, reliable push notifications for high and low glucose alerts matter as much as the readings themselves; FDA has explicitly warned that missed diabetes-device smartphone alerts can create patient safety risk.
For billing, RPM rules still matter: CPT 99454 requires 16 days of data in a 30-day period, so your audit trail cannot be vibes-based. And if your roadmap touches watches or wearable alert surfaces, this is where solid wearable app development starts paying off.
Hypertension Management App Development
A hypertension management app targets the biggest RPM population in chronic care: CDC’s latest figures put hypertension at 119.9 million U.S. adults, or nearly half the adult population. That scale is why this category matters commercially, but the product challenge is not volume alone. It is turning messy home blood pressure monitoring into something a clinician can trust.
What a Hypertension CDM App Must Do Differently
Hypertension is less about novelty and more about disciplined routines. A useful app should guide patients through the standard home protocol: two readings, one minute apart, twice a day, for 3 to 7 days, not random single readings tossed into a chart and prayed over. It also needs to separate home data from office readings so the white coat effect does not distort titration decisions.
The rest is behavioral plumbing. Medication schedules are often multi-drug and time-sensitive. Diet coaching has to connect sodium, weight, and symptoms to outcomes. And because hypertension often travels with other cardiovascular risk factors, smart scale data can add useful context rather than just decorative graphs with ambition.
Device Integration — Hypertension
On devices, Omron and Withings are the names users and clinicians already recognize. Withings offers an official API and device setup SDK; Omron is commonly connected through aggregation layers such as Terra, which can normalize incoming blood pressure cuff data into one pipeline.
The practical rule: support clinically validated cuffs, explain measurement limitations clearly, and design the app around repeated home measurements, not one-off readings. That is where the signal lives.
COPD and Asthma Management App Development
COPD app development sits in a category where the product has to earn its keep clinically, not just cosmetically. The freshest CDC-backed figures put diagnosed COPD at 3.8% of U.S. adults in 2023, while CDC’s latest asthma tables show about 26.8 million Americans with current asthma.
That is why respiratory apps are judged less by step counts and more by whether they help reduce exacerbations, improve adherence, and keep patients out of the hospital.
What a COPD/Asthma CDM App Must Do Differently
COPD and asthma overlap, but they are not twins. Asthma management leans heavily on rescue-inhaler patterns and trigger avoidance. COPD management is more about spotting functional decline and slowing disease progression before it turns into an exacerbation.
In both cases, smart inhaler data is the highest-value signal:
- time of use
- adherence pattern
- sometimes location context
Without that, the app is usually just a prettier symptom diary with aspirations. Commercial respiratory platforms such as Propeller and Hailie exist precisely because medication-event capture is clinically useful.
The next layer is context. Pulling AQI from the public AirNow API is practical, and pairing inhaler events with air quality, weather, or pollen data can make the product more useful. On the clinical side, digital CAT and mMRC assessments should live inside the workflow, not as abandoned PDFs hiding in some menu graveyard.
And if you can ingest spirometry data from a connected spirometer, a pulse oximeter, or the EHR, you get the longitudinal lung-function picture that clinicians actually care about.
FDA Classification — COPD/Asthma
A respiratory app that records medication events is one thing. An app that predicts exacerbation risk for a specific patient is another. FDA’s current CDS guidance makes that distinction more explicit: once your software starts producing patient-specific treatment or risk logic, regulatory scrutiny gets real fast.
That is why alert management needs careful framing. “Air quality is unhealthy for sensitive groups” is safer territory than “use your rescue inhaler now.” The latter starts sounding like clinical advice, because it is.
For related respiratory-device work, this is the same neighborhood as smart inhaler app development.
Heart Failure Management App Development
A heart failure management app lives in the highest-stakes corner of chronic care. The American Heart Association’s latest update still pegs U.S. prevalence at 6.7 million adults, and heart failure remains one of the conditions CMS explicitly tracks under the Hospital Readmissions Reduction Program.
CMS does not do that for fun; it does it because readmissions are expensive and common enough to matter at the system level.
What a Heart Failure CDM App Must Do Differently
Heart failure management is mostly a fluid-status and symptom-surveillance problem. Daily weight is the core signal. The American Heart Association still tells patients to weigh themselves every morning and flag 2–3 pounds in a day or 5 pounds in a week as a warning sign of worsening heart failure.
That is why the app has to enforce a consistent weighing routine and escalate threshold-breaking changes quickly, not bury them in a cheerful chart no one checks.
The second layer is structured symptom capture:
- dyspnea
- orthopnea
- edema
- fatigue
- functional decline
The Kansas City Cardiomyopathy Questionnaire remains one of the most widely used and validated heart-failure patient-reported outcome tools, so this is the right place for daily or periodic PRO collection.
Medication adherence matters too, especially around diuretics and guideline-directed therapy. And because heart failure is a longitudinal disease, the clinician view should track trends in symptoms, weight, activity, and measures such as ejection fraction when available from the EHR or connected devices. A cardiac monitor may add value in select workflows, but the core product is still about actionable longitudinal data, not gadget bingo.
FDA Classification — Heart Failure
This category carries the highest regulatory and liability risk in the guide. Logging weight and symptoms is usually one thing; software that predicts decompensation or recommends therapy changes is another. FDA’s CDS framework is exactly why algorithmic alerting needs regulatory review before launch.
Builder alert: a missed decompensation signal is not a UX problem. It is a patient-safety problem. That is also why heart monitoring app development needs clinical workflow design, not just decent mobile engineering.
Mental Health and Behavioral Health App Development
Mental and behavioral health is one of the largest chronic-care categories. The latest SAMHSA release says 61.5 million U.S. adults experienced any mental illness in 2024, and 52.1% received treatment. CMS also now has established reimbursement pathways for Behavioral Health Integration and the Collaborative Care Model, which makes this a real care-delivery category, not just a wellness app market.
What a Mental Health CDM App Must Do Differently
Mental health apps are harder than they look because the core data is often subjective and the engagement layer is fragile. If a patient drops off, you do not just lose usage. You may lose visibility into worsening symptoms.
That is why symptom capture has to be structured and clinically useful. Validated instruments such as PHQ-9, GAD-7, PCL-5, and MDQ should sit inside the workflow with scoring, trends, and escalation logic. Passive signals from wearables such as sleep, HRV, resting heart rate, and activity can add context, but they should support judgment, not pretend to replace it.
The engagement layer also has to earn its keep. In practice, that usually means:
- evidence-based CBT or behavioral activation content
- crisis coping resources
- secure asynchronous messaging with a therapist or care manager
Regular SMS is not enough. And any team adding AI should think through therapy chatbot compliance before a model starts improvising with vulnerable users.
FDA Classification, Crisis Liability, and Reimbursement
Mental health CDM apps carry two separate risks.
- First, FDA / SaMD risk: software that screens, scores risk, or delivers therapeutic recommendations may cross into regulated territory depending on claims and workflow.
- Second, crisis liability: if your app serves people in acute distress, escalation pathways are part of the safety architecture, not a feature you duct-tape on later. The 988 Suicide & Crisis Lifeline is the national U.S. crisis entry point by call, text, and chat.
On the business side, the key codes remain CPT 99484 for Behavioral Health Integration and CPT 99492–99494 for Collaborative Care Model services. These are not billing trivia. They shape staffing, documentation, and workflow from the start.
Universal Architecture for Chronic Disease Management Apps
A chronic disease management platform is, at heart, a time-series system with clinical consequences. If you model it like a generic CRUD app and promise yourself you will “make analytics prettier later,” later will arrive with a baseball bat.
The architecture has to support longitudinal analysis, device ingestion, provider workflows, and billing from day one. TimescaleDB remains a sensible option because it extends PostgreSQL for time-series workloads through hypertables that automatically partition data by time for faster ingest and queries.

Data Architecture
The safest pattern is boring in the best way:
- store raw readings separately from derived values
- keep condition-specific reference ranges outside the measurement tables
- version your instrument definitions for patient-reported assessments
That means a CGM reading, blood pressure value, or weight entry remains untouched, while trends, risk scores, and summary metrics can evolve without rewriting source data. The same goes for questionnaires: PHQ-9 scoring logic is not something you want hard-wired into one immortal table design.
This is what makes retrospective analysis and regulatory defensibility much less painful. Timescale’s hypertable model is well suited to these range-query and aggregation-heavy workloads.
BLE and Device Integration Architecture
Most device ingestion falls into three buckets: direct Bluetooth Low Energy (BLE) integration, HealthKit or Google Health Connect passthrough, or an aggregation API. For consumer devices such as scales, basic blood pressure cuffs, and some wearable sensor workflows, HealthKit and Health Connect reduce integration overhead and piggyback on Apple’s and Google’s permissions and pairing UX.
Apple supports HealthKit background delivery, and Android’s Health Connect now acts as the system-level health data layer across recent Android versions.
For clinical-grade workflows, though, passthrough is not always enough. CGMs, smart inhalers, or other alert-generating devices often need direct BLE or device-API pipelines because latency, delivery guarantees, and device-specific behavior matter more than convenience.
For broader consumer data such as recovery or activity from Oura, Garmin, or WHOOP, aggregation layers can reduce partnership sprawl. This is the same design territory we deal with in BLE mobile app development, just with higher stakes and less tolerance for “close enough.”
EHR Integration
If the product is meant for clinical deployment, EHR integration is not optional. FHIR API support remains the baseline, with FHIR R4 widely used for exchanging resources like Observation and CarePlan, while SMART on FHIR is the standard launch model for opening an app inside the EHR context.
That is the practical answer to how to integrate with Epic EHR without forcing clinicians into yet another disconnected login.
Alert Architecture and Care Team Dashboard
The patient app may win the demo, but the care-team dashboard is usually the product buyers are actually purchasing. That dashboard should be built around four rules:
- prioritize alerts by clinical urgency, not by timestamp
- make thresholds configurable per patient, not based on population averages
- include documentation for RPM review time and billing workflows
- support offline sync when patient-side connectivity is unreliable
That is the difference between a system that survives real care delivery and one that just looks impressive in a pilot.
Reimbursement Pathways for CDM Apps — The CPT Codes That Matter
A CDM app becomes much easier to sell when the reimbursement path is obvious. For most clinical buyers, that means two core models: RPM reimbursement and chronic care management (CCM).
CMS and HHS guidance make clear that RPM can be billed alongside CCM, BHI, and some other care-management services as long as time is not double-counted.

Remote Patient Monitoring (RPM) — CPT 99453, 99454, 99457, 99458
RPM starts with CPT 99453 for device setup and patient education, then CPT 99454 for supplying the device and collecting physiologic data. The big operational catch is the famous 16-day rule: for RPM data collection, Medicare requires at least 16 days of data in a 30-day period.
CPT 99457 covers the first 20 minutes of treatment management services with interactive communication, and CPT 99458 covers each additional 20 minutes. HHS also notes that the 16-day requirement applies to data-collection codes, not to treatment-management codes 99457 and 99458.
In plain English, a billable RPM workflow needs:
- a qualifying FDA-defined medical device
- electronic automatic data upload
- documented 16-day transmission for CPT 99454
- documented clinical time and interactive communication for CPT 99457 and CPT 99458
Chronic Care Management (CCM) and Behavioral Health Integration (BHI)
For chronic care management (CCM), CPT 99490 covers at least 20 minutes of clinical staff time per month for patients with two or more chronic conditions, while 99491, 99487, and 99489 cover physician time or more complex CCM scenarios. On the behavioral side, CMS continues to support 99484 for Behavioral Health Integration and 99492–99494 for Collaborative Care Model services.
Builder takeaway: your platform needs a real audit trail, not a polite fiction. That is why EHR in medical billing matters here. HHS OIG has repeatedly flagged RPM oversight and improper billing as an enforcement issue, including a 2025 RPM settlement and multiple oversight reports.
HIPAA, FDA, and SOC 2 for CDM Apps — The Compliance Stack
Chronic disease management apps sit where three frameworks overlap, and the expensive mistakes usually happen in the seams.
HIPAA
For CDM products, PHI is everywhere:
- diagnosis context
- medications
- physiologic readings
- symptom logs
- messaging threads
The practical baseline is not abstract. You need a current business associate agreement with every PHI-handling vendor, encryption in transit and at rest, audit logging, and a documented risk analysis process that OCR keeps treating as foundational in enforcement.
That is why HIPAA compliant app development is less about checklists than architecture discipline.
FDA
The FDA question turns on what the software actually does. Passive collection and display may stay outside device scope or fit under the general wellness exemption; patient-specific clinical decision support and treatment-predictive logic are where FDA SaMD, 510(k) strategy, and FDA clearance discussions start showing up in legal review.
FDA finalized updated CDS guidance in January 2026, and its digital health guidance list now also includes the refreshed general wellness policy. For teams building models, health AI FDA clearance is the right rabbit hole to go down early.
SOC 2
Enterprise buyers still use SOC 2 as procurement shorthand for operational maturity. For CDM apps, it should be built alongside HIPAA rather than treated as a sequel.
A serious roadmap should also account for secure software lifecycle expectations that sit adjacent to standards like IEC 62304 and a broader quality management system, especially once the product edges toward regulated-device territory. See also AI in healthcare compliance.
The CDM App Development Process — Phase by Phase
To build a chronic disease management app, you are not sequencing features so much as sequencing risk. The teams that get into trouble usually do one of two things: they start coding before they understand the care workflow, or they treat device access and reimbursement as implementation details. Both mistakes get expensive fast.
Phase 1 — Clinical and Regulatory Strategy (Weeks 1–6)
Start by narrowing the condition, patient cohort, and care setting. A diabetes workflow for endocrinology is not a heart-failure workflow for a health system discharge program. In the same phase, map who actually acts on the data, what the escalation path is, and whether RPM, CCM, or BHI is the economic engine. If a feature starts smelling like prediction or treatment guidance, get the FDA question on the table early, not after design has fallen in love with it.
Phase 2 — Architecture and Device Partnerships (Weeks 6–14)
This is where you decide which data path belongs to which device class:
- direct BLE or device API for alert-generating clinical devices
- HealthKit / Health Connect for lower-stakes consumer device flows
- FHIR R4 and SMART on FHIR for clinical EHR integration
The other non-glamorous truth: developer access for Dexcom, Abbott, and other device ecosystems can take time, so partnership work should start early. This is adjacent to classic IoT app development, except the failure modes are more clinical and less forgivable.
Phase 3 — Development with Compliance Infrastructure (Weeks 14–36)
Build the patient app, clinician dashboard, and documentation workflow together. Do not bolt billing audit trails, encryption, or device validation onto the side later. And test integrations on real hardware, not just simulators. Simulators are lovely until they meet an actual Bluetooth stack and start lying to you.
Phase 4 — Clinical Validation and Launch (Weeks 36–52+)
Pilot with a real cohort, validate outcomes and workflow fit, finalize regulatory documentation if needed, and prepare for enterprise diligence. If procurement is near, SOC 2 Type I often becomes table stakes. And if the product is a regulated medical device, Apple now requires that status to be declared in App Store Connect for relevant markets, including the U.S.
Why Choose Topflight for Chronic Disease Management App Development
Topflight builds chronic care products as operating systems for care delivery, not just patient-facing apps with a dashboard attached. Our work spans the full stack: device integrations, clinician workflows, reimbursement logic, and HIPAA-minded infrastructure.
That includes projects like iFaint, where Topflight built a HIPAA-compliant mobile dashboard for a Stanford-led study, integrating Apple HealthKit and Google Fit data to visualize heart-rate trends and patient-reported symptoms. It also includes Dedica Health, an RPM platform for a cardiology practice with billing reports, time tracking, audit trail, clinically certified sensor integrations, and daily monitoring at scale.
We bring that same approach to every build:
- condition-specific workflow design for real care teams
- integrations across CGM, BP cuffs, smart inhalers, cardiac monitors, and wearables
- FHIR-based EHR connectivity and clinician-facing workflows
- RPM documentation, audit trail, and billing support
- regulatory thinking around alerting and AI-driven features
If you need more than a polished prototype, Topflight can help you build a digital chronic disease management platform that stands up to clinical, operational, and compliance pressure.
Frequently Asked Questions
What features does a chronic disease management app need?
At minimum: device or symptom data capture, trend visualization, alerts, patient engagement tools, clinician workflow support, and billing documentation. The exact mix changes by condition.
How long does it take to build a chronic disease management app?
A realistic first production version usually takes 9–12 months. Device integrations, EHR work, and compliance requirements are what stretch the timeline.
Does a chronic disease management app need FDA clearance?
Not always. Data collection and display may stay outside device scope, but predictive alerts, treatment recommendations, or other clinical decision features can trigger FDA review.
What CPT codes apply to chronic disease management apps?
The main ones are 99453, 99454, 99457, and 99458 for RPM, plus 99490 and related codes for CCM. Mental health workflows may also use 99484 and 99492–99494.
How do I integrate CGM data into a diabetes management app?
Usually through a vendor API, device-specific integration path, or health-platform bridge. The harder part is not fetching glucose data; it is handling latency, alert delivery, and compliance correctly.