
Since the COVID-19 pandemic started, we’ve been receiving a lot of requests to build Teladoc clones. Yes, telemedicine — virtual doctor consultations via video calls — has indeed become a much sought after service.
As a result, many healthcare organizations face a dilemma: to purchase an off-the-shelf telehealth solution or build a custom platform.
In this blog, we’ll show you how these approaches stack up and explain to you how to build a custom telemedicine app like Teladoc in months, even though Teladoc has been around for almost a decade.
Table of Contents:
- Off-The-Shelf Telehealth App Market Overview
- When to Buy a Telehealth Solution
- Comprehensive Analysis: Building vs Buying Telehealth Solutions
- Buy vs. Build: Key Factors to Consider
- When to Build a Telehealth Solution
- The Best of Both Worlds: Customized Platform Solutions
- Silver Bullet to Custom Telehealth App Development: Semi-Custom
- Killer Features of Semi-Custom Telehealth Apps
- How Topflight Makes the “Build” Path the Smart Money Play
- Why Partner with Topflight for Telehealth Development
- Time to Build Telehealth Platform
Off-The-Shelf Telehealth App Market Overview
If I were a CIO of a clinic looking to upgrade its services to telehealth standards, I know for sure it would be a nightmare. There are hundreds of telemedicine solutions on the market to choose from.
If I check the most popular software recommending sites like G2 or Capterra, I’m staring at well over a hundred telemedicine platforms. It’s a tough call to review all of them, let alone try their software to see how it fits our internal workflow — even for an experienced CIO.
At the same time, as someone who deals with telehealth and healthcare app development daily, as I skim through this lengthy list of telehealth products, I can’t see the tools that could help me build my own telemedicine product. Check it out:

Related Article: The Best Telehealth Apps
We’ll talk about how you can leverage those tools despite their absence from the major software catalogues below in section 3.
If you are not familiar with these telehealth enabling vendors, you’re stuck with choosing from other popular telemedicine options like Teladoc, Doxy.me, AmWell et al.
Before you rush to read user reviews on popular telemedicine platforms to see how they align with your work processes, let’s see if a custom-built telehealth platform is a better alternative.
When to Buy a Telehealth Solution
Evaluating Off-the-Shelf Platform Limitations
You’re not buying a feature list; you’re buying constraints. Run this quick filter:
- Workflow fit: Can intake → routing → documentation run without workarounds?
- Data model: Custom fields, role-based permissions, and reporting grains—fixed or flexible?
- Roadmap control: Can you pin versions and schedule upgrades, or do releases pick you?
- Auditability: Immutable logs, rationale exposure, and export on demand—or PDF comfort blankets?
- Scalability: User caps, rate limits, visit concurrency—published or “contact support”?
- EHR/PM coverage: Native connectors vs. “on our roadmap.”
If 20% of your flows are non-standard, prebuilt friction will feel like 80% of your day. Buy only if you can live inside the opinionated box. Platforms are fast until their guardrails become your guard dogs.
Hidden Costs of Pre-Built Solutions
Sticker price is the appetizer; the MSA is the entrée:
- Per-visit/minute/provider fees that scale faster than revenue
- Premium gates (SSO/SCIM, advanced analytics, audit exports)
- Change orders for “tiny” tweaks (extra intake fields, routing logic)
- Data egress/migration charges when you want warehouse freedom—or to leave
- Forced-upgrade costs (re-testing, retraining) and “premium support” tiers
- White-label/branding limits that quietly add design debt
Model 24–36 months, not month one. If growth is the plan, rent will outpace the mortgage. Budget the way out as carefully as the way in.
Integration Challenges with Existing Systems
Where good intentions meet HL7:
- Coverage gaps: Partial FHIR objects, brittle HL7 bridges, and version drift with your EHR/PM
- Eventing: Missing webhooks/callbacks → polling and reconciliation headaches
- Identity & matching: MRN/portal accounts/dup detection—who’s source of truth?
- RCM rails: Scheduling, eligibility, charge posting—idempotency or double-book/ double-bill risk
- Testing reality: Sandbox ≠ prod; no synthetic PHI strategy ⇒ slow QA, surprise failures
Mitigate up front: require published version matrices, error taxonomies, idempotent APIs, and a documented exit ramp (full data + labels export). If those are “roadmap,” that’s your risk, not theirs. If integrations are “coming soon,” assume “not soon enough.”
Comprehensive Analysis: Building vs Buying Telehealth Solutions
We often hear from our customers that they have to rely on several standalone applications to get meaningful telehealth going at their practice. So in most cases, this setup includes at least an EHR system integration and a telemedicine solution.
However, even though that approach was a no-brainer in the early COVID-19 days, providers do need a more straightforward experience now, with less jumping between different systems.
What will you gain or lose if you replace this combination of a standalone telemedicine app plus EHR with a unified off-the-shelf telemedicine product or build one from scratch?
Pricing
Let’s face it, an off-the-shelf telemedicine application will cost you less in the short-term perspective. However, subscription and transactional payments, which have become ubiquitous, will inevitably surpass the upfront investment you need to make when developing a custom telehealthcare solution.
Ready-made telehealth vendors may charge per minute, per provider, or offer a flat monthly fee. Regardless of their model, you’ll be paying every month, ratcheting the overall cost of the telemedicine system higher and higher. And this accumulative effect will start to add up when your practice begins to grow.
Here’s how we project the cost of ownership for custom vs. built telemedicine application can vary over time for a mid-sized practice with 20 clinicians, growing at a reasonable pace:
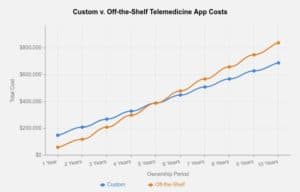
Remember that you also need to factor in support costs (for providers and patient assistance), plus your personnel will need to learn how to use the new shiny tool.
TLDR: the cost is more affordable for custom-developed telehealth apps, although the upfront investment is higher than an off-the-shelf solution, which starts to snowball over time.
Related: Understanding App Development Costs: Budgeting for your App
Features
In terms of functionality, both off-the-rack and custom-built telehealth apps can be quite similar. However, what happens in practice quite often is you get more features than you’re actually using with a ready solution (think of the 100’s of cable channels that you pay for but never watch!)
One other disadvantage of such one-size-fits-all telehealth solutions is that you depend on them to integrate with other medical systems you use on a daily basis. And if the vendor does not support integration with your particular EHR or practice management system, you’re out of luck.

Custom-built telemedicine apps are great in that respect because you get to choose what features will be there. Moreover, even if you’re not building all of them at once, you can ask your telemedicine developer to create an app architecture allowing further upgrades.
TLDR: you get the exact features you need and integrations with a custom solution, whereas a canned telemedicine platform would always come with something extra you don’t need and may miss a few things than you need.
Related: Everything you need to know to build your own telehealth solution
Branding
Of course, if you pay for a ready-made telehealth system, it will offer some sort of branding. One thing to keep in mind, though, is that you don’t decide how that would translate to your customers.
In other words, it may well be just a logo slapped onto an otherwise completely generalized interface, used by everybody else.
As you can imagine, your only limitation is imagination and the UX/UI acumen of the team that assists you when it comes to developing your own system.
TLDR: limited vs. unlimited branding opportunities for canned and custom telehealth apps, respectively.

Business model fit & sustainability
Another aspect worth considering when choosing between a custom and off-the-shelf platform for remote healthcare services is how the whole thing fits in your business model.
Do you see this telehealth app as the primary revenue stream for your practice, or do you want to run it as a value-added service?
It can certainly become scary if telehealth is your main revenue source, and you totally depend on a third party with its maintenance and upgrades. What happens with your practice if the vendor goes out of business or gets acquired by a bigger company?
TLDR: if telehealth is an add-on service worth considering an off-the-shelf solution, otherwise way less risky with a custom-built app.
Discover the elements that contribute to the average cost of EHR systems in our comprehensive blog post.
Go-to-market pace
There’s no arguing that with an off-the-shelf telemedicine app, you get to start faster. Not immediately by any means as you still need to set up servers and tune everything up, but still much faster than developing a custom system, which easily takes six months or longer.
The reason why it takes this long to build a custom platform is that it will be 100% tailored to your existing workflow. To achieve this, telemedicine developers will need to start with a prototype tested in a real environment and optimized before coding begins.

However, prototyping is just the tip of the iceberg. Development and testing will take up the chunkiest lump of the implementation process.
EXPLORE OUR RAPID PROTOTYPING SERVICES
What’s interesting is that with a ready telemedicine app, you’ll face issues when trying to update it with new features. It will be easier to do with a custom solution because you will fully control its source code.
TLDR: Faster with a ready-made telehealth tool, but with the custom approach, you can grow faster down the road as your customer base begins to grow.
“We’ve practiced telemedicine for years, but the technology that’s available now for patients to access and communicate with primary care doctors or specialty doctors is so exciting. It’s so great at this point in time that the board has to address this. I mean, it’s the wave of the future for medicine.”
Dr. Steve Magie, Ophthalmologist
Buy vs. Build: Key Factors to Consider
Total Cost of Ownership Comparison
Sticker price lies; 36-month TCO tells the truth.
Off-the-shelf (Buy): Lower upfront, then the meter runs—per-provider/visit/minute, premium add-ons (SAML/SCIM, advanced analytics), integration change orders, and data-egress if you ever want your raw events somewhere useful.
Custom (Build): Higher day one (engineering), then predictable run costs (hosting, monitoring, updates you control). As volume grows, you’re not paying a tax on every incremental success.
For a mid-sized practice (≈20 clinicians, steady growth), Buy usually wins Year 1 (cash outlay), then loses Years 2–3 as fees compound—especially if you’re paying for bundles you never fully adopt. Custom catches up because you’re investing in assets, not renting toggles.
Don’t forget support gravity (provider/patient help desk), training, and the “roadmap tax” when a vendor’s priorities aren’t yours.
TL;DR: If telehealth is strategic revenue, TCO converges fast—and owning the code compounds in your favor.
Customization Flexibility Assessment
You can either bend workflows to a template or shape the template to your workflows.
Off-the-shelf: Opinionated UX, fixed data models, and “almost what we need” intake/triage that accumulates workarounds. You inherit someone else’s integration shortlist and release cadence.
Custom: Encode the exact intake logic, roles/permissions, and visit routing you live and die by. Keep the architecture extension-friendly (feature flags, module boundaries) so Phase 2 isn’t a rebuild.
Heuristic from the trenches: if ≥20% of your flows are non-standard, you’ll feel 80% of the pain inside a rigid platform. Every workaround becomes a training problem, then a quality problem.
TL;DR: Templates are fast until they aren’t. Flexibility pays for itself the moment your clinic isn’t average.
Time-to-Market Analysis
Speed now vs. speed later—the trade nobody likes to say out loud.
Off-the-shelf: Pilot in weeks once legal/BAA/branding/integrations clear. Great for dates on a board and board slides. But post-pilot, every tweak is a ticket (and a wait).
Custom: MVP in months, not quarters, if you stage scope ruthlessly: nail intake → visits → notes → billing rails. After launch, change velocity is yours—no vendor queue between you and an improvement.
A practical split: buy to prove demand fast; build to scale without handcuffs. Most teams regret not switching earlier once the pilot graduates to real volume.
TL;DR: Buy to hit the first date. Build to hit every date after.
Compliance and Security Implications
Compliance isn’t a PDF; it’s an operating mode.
Off-the-shelf: You get a BAA and inherited attestations—good start. Ask for version pinning, rationale exposure (why a decision was made), immutable audit logs, and data export on demand. If those are “roadmap,” your risk lives on a Gantt chart.
Custom: You set PHI boundaries, log every action (who/what/why/version), and ship HIPAA-first defaults (encryption, least-privilege, breach workflows). Third-party comms (SMS/video) can be HIPAA-ready—your architecture decides whether they actually are.
Non-negotiables either path: consent tracking, auditable change history, kill-switch/rollback, and monitoring that pages a human before the OCR guy on Twitter notices.
TL;DR: Buy reduces paperwork fast; build reduces blind spots long-term. The safest system is the one you can actually change intentionally.
If telehealth is strategic—not a side gig—here’s when build beats buy (and how to prove it on a spreadsheet, not a slide).
When to Build a Telehealth Solution
When to build? When telehealth is a core revenue line—not a side quest—and your workflows aren’t “template-shaped.” If per-visit pricing quietly eats margin at scale, your EHR/PM landscape is… creative, governance requires auditability you can actually change, and you need roadmap control (version pinning, fast iterations, real export), building stops being risky and starts compounding.
The only adult move before green-lighting is math: quantify fees you’ll stop paying, clinician minutes you’ll stop wasting, and revenue you’ll stop leaving on the table—then compare that to what it costs to run and evolve the thing. That’s your go/no-go. Now, let’s make it explicit.
Custom Development ROI Calculator
You don’t green-light on vibes—green-light on payback.
Inputs to model (monthly):
- Visit volume × (platform fees avoided per visit)
- Clinician minutes saved/visit × fully-loaded cost/minute
- Reimbursement uplift from better documentation/compliance
- Minus: cloud/inference, monitoring/SRE, support, release QA
Formulas:
- Net benefit/month = (fees avoided + labor savings + revenue lift) − run costs
- Payback (months) = upfront build cost ÷ net benefit/month
- Year-1 ROI = (12 × net benefit − amortized build) ÷ amortized build
Rules of thumb:
-
If telehealth is strategic revenue and payback ≤ 12–18 months, build is usually the safer bet.
-
If telehealth is ancillary and payback > 24 months, buy or hybrid first, then refactor to own later.
Ship what improves the model; punt nice-to-haves to Phase 2 so the math stays honest.
Building with Topflight vs In-House Development
In-house: hiring runway, compliance learning curve, context switching with internal priorities, retention risk mid-build.
Topflight: healthcare-native UX, HIPAA-first pipelines, EHR marketplace experience, and reusable components that compress hours to MVP—while you keep the source and roadmap control.
Pragmatic split we recommend:
-
Topflight lays the rails (intake → visit flow → notes → billing hooks, audit, monitoring).
-
Your team owns day-2 ops and clinic-specific iteration.
Phased Development Approach Benefits
Speed without self-harm. Prove value early; scale intentionally.
Phase 0 — Discovery & Guardrails
KPIs, roles/permissions, PHI boundaries, audit spec.
Phase 1 — MVP (one specialty/flow)
Must-haves only: intake → scheduling → visit → documentation; basic analytics.
Success = time-to-visit cut, fewer no-shows, NPS ≥ target.
Phase 2 — Scale & Integrations
EHR/PM depth, eligibility/RCM rails, richer reporting, white-label options.
Success = lower admin minutes/visit, clean claim rates, stable concurrency.
Phase 3 — Optimization & Hardening
Performance, cost tuning, versioning/rollbacks, SSO/SCIM, full audit exports.
Success = predictable release cadence and “boring” ops.
Why this works: it matches your semi-custom narrative and makes later sections (features, case studies) the obvious next click.
The Best of Both Worlds: Customized Platform Solutions
When “buy” gets you live fast but “build” is how you win long-term, go hybrid: keep the platform you like, then layer the workflows, rails, and safeguards you actually need—without forfeiting code ownership or HIPAA-first patterns. Think of us as telehealth solution architects who turn a good platform into your platform.
How Topflight Enhances Off-the-Shelf Platforms
We remove vendor handcuffs—no waiting on a backlog.
- Workflow fit, not workarounds: Custom intake/triage, roles/permissions, and visit routing that mirror your clinic.
- Audit & governance that sticks: Immutable logs, rationale exposure, version pinning, export-on-demand.
- Performance & UX hardening: Concurrency tuning, NPS-friendly UX, and a release cadence matched to your ops.
- AI where it earns minutes back: Ambient notes, coding assist, triage summarization—implemented with HIPAA-safe patterns.
Custom Integration Services for Telehealth
Your platform is only as good as its rails. We wire those rails—end to end—as part of our healthcare technology consulting services:
- SMART on FHIR & HL7v2: Clean read/write, eventing, idempotent scheduling (no double-books or double-bills).
- EHR marketplace onboarding: Epic Connection Hub, athenaOne, etc.—submission → sandbox QA → listing.
- RCM & identity flows: Eligibility, claims, charge posting, MRN matching—aligned to your source of truth.
- Regulatory posture baked in: HIPAA controls from design → deploy, with ongoing compliance support.
White-Label Telehealth Development by Topflight
Prefer your brand on the door—and your code in your repo? We assemble on Specode, an automated platform with reusable HIPAA-compliant components (telehealth, scheduling, messaging, intake, notifications), then tailor and ship under your label. You keep the source; we keep the velocity. Three on-ramps: self-serve via Specode’s AI assistant, hybrid (AI + expert code), or full-service by our team—switch paths anytime.
Silver Bullet to Custom Telehealth App Development: Semi-Custom
At Topflight, when we build a custom telehealth solution, we are not building everything from scratch. I bet very few people do this because if you think about it — you need to develop Skype with a healthcare window dressing. And it certainly took a while to build Skype.
Instead of building a HIPAA compliant custom audio/video teleconferencing backbone, we use existing technologies like Agora.io or Twilio. Those are well-established companies with outstanding communication platforms that they offer as pluggable components.

So when we build a telemedicine app, we mostly focus on the UI and streamlining of your workflows and then plug user-facing features with Agora’s back-end. This back-end is where audio and video calls really take place.
Besides the telecom aspect, we do use other shortcuts where possible to fasten your time to market and lower the cost of developing a telemedicine app:
- authorization (OAuth 2, OpenID)
- patient scheduling (Acuity, Calendly)
- payments & billing (Stripe, 2CheckOut)
- e-prescribing (Dosespot, MD toolbox)
What remains fully customizable is user experience, and it’s what matters most. At the same time, we rely on proven partnerships to add seamless telecom features. That’s why we call our approach semi-custom development.
We use these SDKs and APIs as a kind of building brick to build your telemedicine app faster, without the need to reinvent the wheel. It’s also worth noting that such custom solutions will integrate with your existing EHR system and other practice management tools, which is not always guaranteed with off-the-shelf telemedicine applications.
Related article: How to Build an Electronic Medical Record System (EMR or EHR)
Killer Features of Semi-Custom Telehealth Apps
Let’s wrap up by outlining features you can get only if you go with a semi-custom telehealth app. What unique advantages do you get in this case?
Full transparency and cost predictability
With a custom platform, you get a complete per-feature cost breakdown. So you can decide what features to implement first and which can be added later. On the contrary, you pay for the whole package with off-the-shelf, including stuff you won’t use anyway.

White-label your solution to others
Like it says, you can white-label your own solution to other clinics and providers on your terms. It’s like running your own Teladoc and controlling its future.
Out-of-the-box HIPAA Compliance
Another bonus of building a custom telemedicine app is that most third-party call-enabling tools (like Agora.io or PubNub) will feature out-of-the-box HIPAA compliant development.
This effectively means that your development team will spend less time optimizing around the app’s security and more time building its features. All communication through such custom telehealth apps, including audio and video calls and chats, will protect PHI.
Be the pioneer
Before an off-the-shelf vendor decides to add, let’s say, an Apple Watch support, it will take a market shift — they need customers to start really demanding an Apple Watch app. With telehealth app development, nothing prevents you from experimenting and adding new features and supporting new cool hardware, not necessarily throwing a bunch of money at it, but still having this opportunity to innovate.
How Topflight Makes the “Build” Path the Smart Money Play
Choosing to build your telehealth stack only pays off if you can ship fast and hit clinical KPIs out of the gate. That’s exactly what we did for RTHM—a Long-COVID RPM platform that went from whiteboard to multi-platform MVP in ≈1,400 engineering hours, thanks to a low-code back end plus our custom patient and provider apps. When Allheartz needed computer-vision rehab on mobile, our six-month, 800-hour MVP cut in-person visits 50 % and shredded clerical grunt work 80 %—proof that speed and outcomes can coexist.
Those wins sit alongside more than $188 million in follow-on funding raised by products we’ve engineered, a stat we splash right on our homepage because investors keep voting with their wallets . Bottom line: if your buy-vs-build debate hinges on budget, timeline, and traction, Topflight has receipts that say “build”—with us—is the safer bet.
Why founders pick Topflight for telehealth builds
-
Sprints, not marathons – Cross-platform React / React Native codebases and reusable HIPAA-ready modules get you to pilot while competitors are still scoping.
-
Outcome-driven UX – Built-in analytics for visit reduction, engagement, and reimbursement make CFOs and VCs purr.
-
Compliance baked in – HIPAA, SOC 2, and PHI encryption from sprint one—no eleventh-hour security tax.
-
EHR & marketplace savvy – Epic Connection Hub, Athena Marketplace, SMART-on-FHIR… we’ve cleared every gatekeeper without déjà-vu resubmissions.
Why Partner with Topflight for Telehealth Development
You’re not picking a vendor; you’re picking an operating model. Our lane is custom telehealth platform development that ships fast, integrates cleanly, and stays compliant—without locking you into someone else’s roadmap.
DIY vs Vendor vs Topflight Custom Solution (Specode)
|
Decision Lens |
DIY (In-House) |
Vendor (Off-the-Shelf) |
Topflight + Specode (Custom) |
|---|---|---|---|
|
Speed to pilot |
Slow hiring + context switching |
Fast once BAA/branding clear |
Fast: reusable components + focused build |
|
Control & roadmap |
High, but bandwidth-bound |
Low; you inherit their backlog |
High; you own code + we accelerate |
|
Integration depth |
Depends on team experience |
Limited to supported connectors |
FHIR/HL7 rails, RCM flows, idempotent APIs |
|
Compliance posture |
You learn by shipping |
BAA + attestations, opaque internals |
HIPAA-first defaults, auditable by design |
|
Long-term TCO |
Good if you retain talent |
Fees compound with volume |
Invest once, predictable run costs |
|
Change velocity |
Competes with other priorities |
Ticket → wait → release window |
Your cadence; we ship, you iterate |
|
Data ownership |
Yours (if you build it right) |
Often gated/egressed |
Yours, warehouse-ready, version-pinned |
|
Exit cost |
Low (you own it) |
High (migrations, fees) |
Low (no lock-in, clean exports) |
Net: DIY maximizes control but burns calendar; vendors win week one and tax you forever; Topflight + Specode keeps the speed and hands you the keys.
Why Partner with Topflight for Custom Development
- Healthcare-native product craft: Intake → visit → notes → billing designed around clinician minutes saved, not feature bingo.
- Integrations that survive Mondays: SMART on FHIR + HL7v2, eligibility/RCM, scheduling with dedupe keys, clear source-of-truth mapping.
- Security you can audit: Immutable logs, rationale exposure, version pinning, export-on-demand—delivered by HIPAA-compliant telehealth developers.
- Semi-custom velocity with ownership: We assemble on Specode’s reusable HIPAA-ready components, tailor what’s unique, and you keep the source and roadmap.
- Operational rigor: Monitoring, alerting, rollback paths, and safe release trains so “go-live” isn’t code for “hold your breath.”
- ROI-first delivery: Phase what moves the model (fees avoided, minutes saved, reimbursement lift); everything else waits behind a flag.
If you want the speed of a platform and the leverage of owning your stack, this is the path that compounds.
Time to Build a Telehealth App?
Remember that when you buy into a ready-made telemedicine app, you’re just like everybody else — you’ve got the same features to show, the same interface, etc. On the other hand, if you develop a custom telehealth application, you get to be unique and carry over unique benefits to your customers.
How Topflight Helps You Make the Right Decision
We run a fast, evidence-based decision sprint—no slideware, just numbers and a working path. In 10–14 days you’ll know whether buy, build, or hybrid wins for your clinic and why—complete with a phase plan you can take to your CFO (or your board).
If “buy” wins, we harden the platform you chose. If “build” wins, we scope the smallest shippable that pays back fast. Either way, you keep all artifacts.
- 36-month TCO + payback model using your visit volume, staffing, and fee assumptions.
- Integration feasibility map (EHR/PM, identity, RCM) with risks, mitigations, and test plan.
- Compliance & audit blueprint (BAA needs, logging spec, version pinning, export-on-demand).
- Clickable prototype of intake → visit flow to validate with clinicians before code.
If you have questions about creating a telemedicine solution and taking advantage of a 90% discount on HIPAA-compliant video calls through our partners, get in touch.
Related Articles:
- A Guide to Chatbots in Healthcare
- How to build an Mhealth Application
- A Guide to Healthcare App Design
- Medical Website Development Guide
- How to Start a Healthcare Startup
- Doctor Appointment App Development
- ePharmacy App Development Guide
- Mental Health App Development Guide
Frequently Asked Questions
Do Agora.io, Twilio, or similar health enabling tools ship as part of a patient or doctor-facing interface?
No, these tools provide the technology for healthcare app developers to enable out-of-the-box HIPAA compliant video calls in a telemedicine app.
Will a custom telemedicine solution work with my existing software like EHR?
In 99% of cases, yes. Your telemedicine app developers will require APIs for your existing solutions (which they practically always have), or find some other workarounds.
Can you provide a ballpark estimate to build a telemedicine app?
No, we will need to find out the features you envision for your patients and doctors. The cost will also depend on what platforms you want to support: web/iOS/Android. To give you a number out of the blue, $60K should get you started on the MVP path.