
A billion-plus people worldwide live with a mental health condition right now, and the supply side isn’t catching up. Therapist waitlists run weeks to months, crisis lines stay stretched, and primary care isn’t built to absorb the overflow. That’s where mental health apps land, and that’s the category we’ve been building into for the better part of a decade.
This guide is what we’d hand a founder or PM walking into mental health applications development cold. What types of apps are getting funded right now, what HIPAA-compliant looks like beyond the BAA checkbox, real cost ranges from projects we’ve shipped, and the specific traps that turn a 6-month build into 14 months. If you’re developing an app for mental health and have a therapist or clinician on the team, even better. Most of what’s in our portfolio came out of those conversations.
How do you build a mental health app?
Pick the type first, since type sets the regulatory load: a meditation app and a teletherapy platform are different builds. From there, the floor is HIPAA (or the FTC’s health-data rules for D2C apps outside it). Scope the MVP around one core job instead of all 7 features. Budget $70,000 to $140,000 and 4 to 6 months for a HIPAA-grade build.
Key Takeaways:
- Mental health app development splits into 7 types, and the type you pick sets the regulatory load. A mood tracker and a teletherapy platform sit at opposite ends of that load, and everything downstream follows from the first call.
- Compliance decides what you’re allowed to ship. HIPAA is the floor when PHI and providers are involved; D2C apps outside it answer to the FTC’s health-data rules instead. Sort this out before the feature list.
- The 2026 bar is state AI-therapy law. Illinois, Nevada, Utah, California, and Texas regulate AI in the care loop, with more states copying the text; an AI feature now carries its own legal review.
- A HIPAA-grade MVP runs $70,000 to $140,000 and 4 to 6 months. Built right, the category pays: since Topflight Apps took over Soberbuddy, retention is up 300% and funding has reached $1.25 million. Our lead AI architect’s read on that turnaround: “The first AI decision on Soberbuddy was removing the AI. The previous team had strapped machine learning onto a product that had no job for it, and the numbers only started moving once we stripped it out and rebuilt around the CBT core. That lesson aged well: in 2026, a model either earns its place in the care loop or it’s pure risk.“
Mental health app development at a glance:
| Typical MVP cost | $70,000 to $140,000; blended-care platforms run $200,000 and up |
| Timeline | 4 to 6 months for a HIPAA-grade MVP; about 3 months for a wellness build with no PHI |
| Lowest-regulation entry | Self-management and meditation apps |
| Highest-regulation builds | Teletherapy and crisis intervention apps |
| Compliance floor | HIPAA with signed BAAs, or the FTC’s Health Breach Notification Rule for D2C apps outside HIPAA |
| 2026 watch item | State AI-therapy laws: Illinois, Nevada, Utah, California, and Texas, with more states copying the text |
Table of Contents:
- Mental health applications development matured into clinical infrastructure in 2026
- The seven types of mental health applications carry very different regulatory loads
- Mental health app compliance and privacy requirements decide what you’re allowed to ship
- Must-have mental health app features (and why you shouldn’t build all 7 in v1)
- Integrations that make a mental health app actually useful
- Creating a mental health app delivers four results you can measure
- Monetization strategies for mental health applications are trust decisions first
- The key aspects of mental health app development get decided before the Gantt chart
- Step-by-step guide on how to create a mental health app, one decision per step
- The tech stack for mental health apps is downstream of three decisions
- 10 takeaways from negative reviews on mental health apps (we’ve read them so you don’t have to)
- The key challenges in mental health app development sit between the what and the how
- Mental health app development cost starts around $70,000 and climbs with scope
- The future of mental health app development looks like infrastructure
- Topflight Apps’ experience with mental health app development, in four shipped products
Mental health applications development matured into clinical infrastructure in 2026
Behavioral health app development matured into clinical infrastructure in 2026: the products that win now integrate with real care delivery, carry clinical evidence, and increasingly get reimbursed.
Market growth and investment signals are strong, and the bar rose with them
If you’re going to make an app to help with mental health, demand is the easy half of the pitch. More than 1 billion people worldwide live with a mental health disorder, anxiety and depression first among them, by WHO’s latest count. Supply keeps failing people with mental health problems the same way: appointments run weeks out, and care doesn’t stick between sessions. That’s the mental health care gap.
A mental health app fits that gap directly. Someone who’d wait three weeks for a therapy slot can open one today and get a CBT module, journaling prompts, a peer-support thread, or async messaging with a clinician. For founders, that mix of unmet need and growing reimbursement is rare in digital health: one of the few categories where you can hit a public-health number and still run a real P&L.
The clinical receipts are finally landing. In March 2025, Dartmouth published the first randomized controlled trial of a generative AI therapy chatbot. 210 adults with major depressive disorder, generalized anxiety disorder, or eating-disorder risk got 8 weeks with Therabot or a waitlist:
- depression symptoms dropped 51%
- anxiety reduced by 31%
- eating-disorder body-image concerns dropped 19%
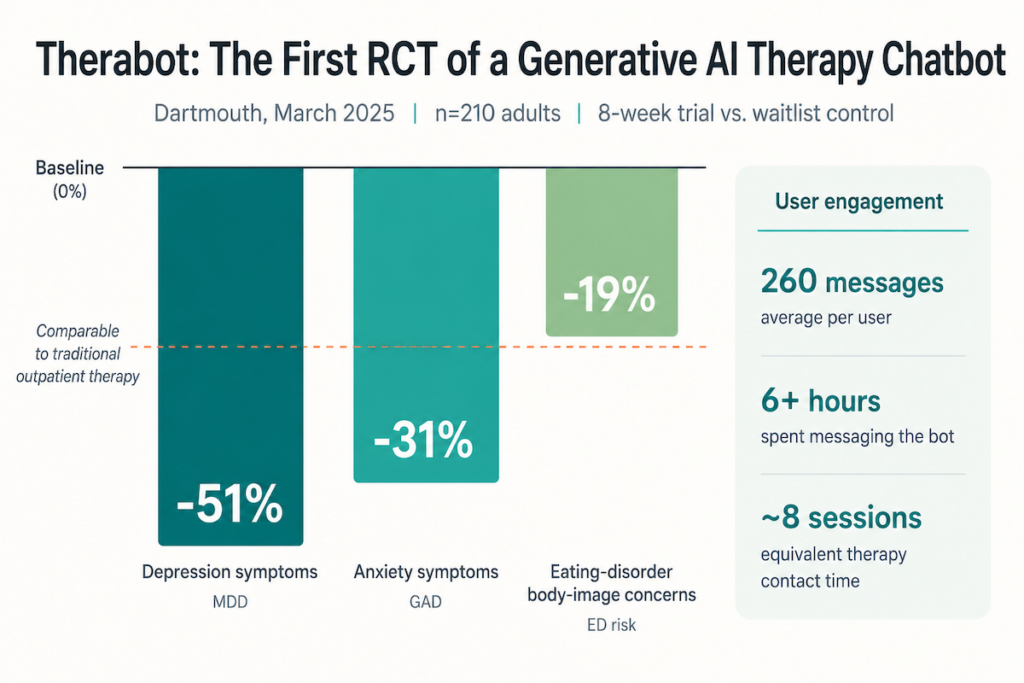 The average user sent 260 messages and spent over 6 hours messaging the bot, roughly 8 therapy sessions worth of contact. Dartmouth called the improvements comparable to traditional outpatient therapy, the highest evidence bar the category has cleared.
The average user sent 260 messages and spent over 6 hours messaging the bot, roughly 8 therapy sessions worth of contact. Dartmouth called the improvements comparable to traditional outpatient therapy, the highest evidence bar the category has cleared.
On the system side, these tools are getting woven into crisis care pathways, youth mental health programs, overdose prevention initiatives, and broader behavioral health services. The “consumer wellness” framing is dated. As more counseling apps get evaluated and folded into real care delivery, the category starts to look like infrastructure.
Zoom out to the broader digital mental health category (apps plus enterprise behavioral platforms, clinician marketplaces, and employer benefits) and the market is forecast to grow from about $33 billion in 2025 to more than $150 billion by 2034.
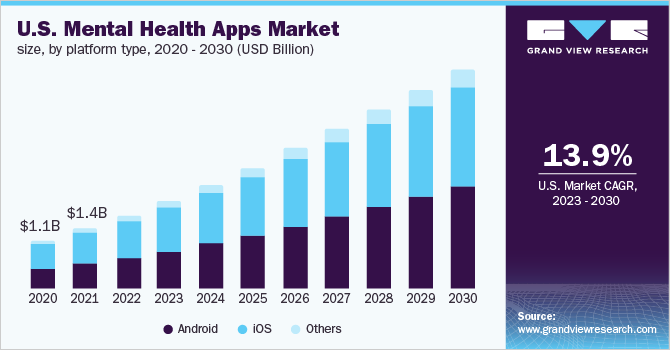
U.S. mental health apps alone were a $1.4B market in 2021, and the segment is forecast to compound 13.9% a year through 2030.
Image credit: Grand View Research (all rights belong to Grand View Research, Inc.)
Funding tells the same story. Per Galen Growth’s 2024 year-end count, mental health now pulls in roughly 12% of all digital health investment worldwide, about $2.7 billion across 184 deals, up 38% year over year. In the U.S., digital health funding overall rebounded to $14.2 billion in 2025, up 35% over 2024 and the highest total since 2022, according to Rock Health’s year-end report published in January 2026. Investors keep writing checks even as capital concentrates in fewer, larger rounds, with mental health one of the recurring theses in those portfolios.
COVID-era urgency was supposed to be the driver, but app usage stayed elevated long after the pandemic surge. Reimbursement experiments and enterprise contracts replaced the early tailwind, and the “therapy uberization” trend (on-demand access and async support) is sticking around. What changed across the mental health industry by 2026 is the bar. The win condition now is clinical credibility and real integration with care delivery. Launching an app doesn’t make you a player anymore.
The payer side is moving too. In November 2024, CMS approved three new reimbursement codes for FDA-cleared digital therapeutics covering Medicare patients. In September 2025, Cigna became the first major commercial insurer to follow, announcing coverage for FDA-approved digital therapeutics. And in November 2025, the CY2026 Physician Fee Schedule widened the Medicare codes to FDA-authorized ADHD devices, effective 2026.
Those Medicare codes only reach the small set of devices that cleared FDA, and for that set, the business model stopped being subscriptions alone. If you’re building toward an FDA submission, the path to reimbursement is now less hypothetical than the path to a working product.
The opportunity is real. Breaking in credibly is harder than it looks, and a few numbers are worth holding onto before you build:
- An estimated 10,000 to 20,000 smartphone mental health apps sit in major app stores, per the American Psychological Association and One Mind PsyberGuide. New ones appear and disappear constantly, so the visible slice of the mobile app market churns month to month
- Most of them have no clinical evidence behind them. A 2025 systematic review in Internet Interventions, based on the MIND app-evaluation database, found only ~15% of general mental health apps have any feasibility or efficacy study, and a 2020 review in JMIR mHealth and uHealth (Lau et al.) pegged the share with published, peer-reviewed research support at about 2%.
- Only about 7% of people with mental health or substance use disorders worldwide receive effective treatment, per a February 2025 JAMA Psychiatry analysis of WHO World Mental Health Survey data across 21 countries. Mobile apps are one of the few realistic ways to reach the rest with support for depression, anxiety, and suicidality risk.
- Adverse-event reporting is bad. A December 2024 systematic review in npj Digital Medicine (Linardon and colleagues) found only 55 of 171 trials involving mental health apps reported adverse events at all. That’s why safety monitoring and escalation paths belong in the build from day one, not retrofitted after the first incident.
- Between 2011 and 2030, the global economic output loss from mental disorders is projected at $16.3 trillion, per a 2011 World Economic Forum and Harvard School of Public Health study. The case for digital mental health infrastructure isn’t a 5-year story.

The bar moved in 2025 because regulators finally noticed.
- August: 44 state attorneys general sent a formal letter to Google, Meta, and OpenAI demanding safer chatbot products for minors.
- September: the FTC opened a formal inquiry into the same companies, and APA testified before the Senate Judiciary Committee urging Congress to make it illegal for any chatbot to pose as a licensed professional.
- By November, APA had issued its first formal health advisory warning that engagement with GenAI chatbots and wellness apps for mental health can “have unintended effects and even harm mental health.”
- In January 2026, Character.AI settled multiple lawsuits brought by parents of teens who died by suicide or attempted self-harm after extended chatbot use.
Table stakes for any consumer-facing mental health app shipping in 2026: pre-deployment safety testing, real crisis pathways, age-appropriate gating, and no AI-as-therapist framing without licensure. The companies that built to that bar from day one are about to look smart.
Mental health app development has four advantages that rarely co-occur
Why build a mental health app at all? Four forces line up in this category that rarely line up together elsewhere in digital health: demand outstrips supply for mental health applications, reimbursement is finally catching up, product value compounds with engagement, and the regulatory bar is high enough to create real defensibility for whoever clears it. Most digital-health categories have one or two of those. Mental health has all four.
| Reason | Why it matters in practice |
|---|---|
| Accessibility | Apps clear the geography and scheduling barriers that knock people out of care before they start. The reach goes deepest in rural counties and underserved zip codes, where the nearest in-network psychiatrist can be hours away. |
| Cost economics | Per-user economics improve as you load more users onto the same backend, which is why nearly every consumer mental health app moved to subscription pricing early. The marginal cost per active user keeps dropping past the break-even point; clinic models can’t match that curve. |
| Privacy by default | Stigma keeps a real share of people out of therapy. An app is private by default: no building to walk into, no clinician’s office hours to schedule around, no explaining to a partner where you’re going on Wednesday nights. That privacy reaches the population that wasn’t seeking care in the first place, which is half the unmet-need story. |
| Personalization that earns its keep | ML lets you do things at the user level that clinicians can’t do across thousands of patients: spotting when a check-in pattern shifts, or routing someone to a clinician when their PHQ-9 score crosses a threshold. That personalization is what keeps people in the app past week 3, where most consumer health apps lose them. |
| Engagement signal as a moat | Engagement signals tell you which interventions are actually working and where users are churning. Healthcare apps that ignore this signal layer get out-iterated by ones that don’t, and the gap compounds over years. |
Now to the types of apps actually getting built.
The seven types of mental health applications carry very different regulatory loads
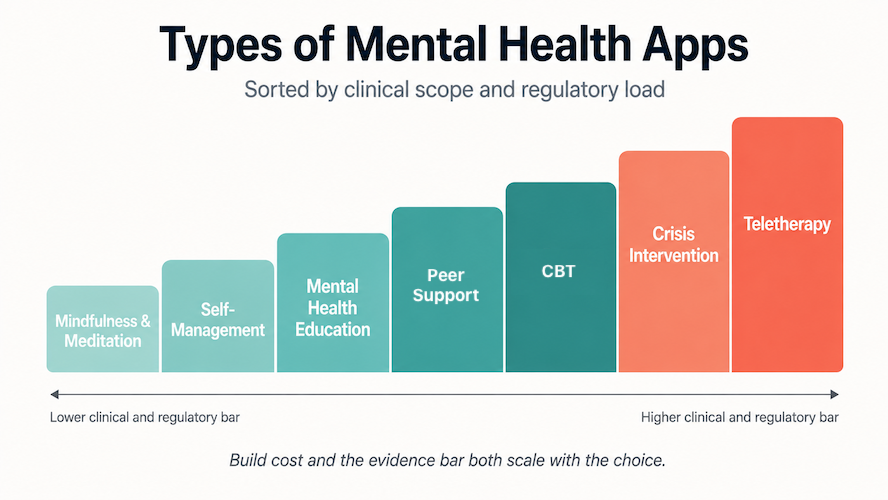
Mental health apps fall into seven types, and each type carries a different clinical scope and regulatory load. The seven categories below cover what’s actually getting built and funded in 2026. The lines blur in practice: a peer-support app that adds CBT modules becomes a CBT-plus-community app, and most teletherapy platforms ship with self-management features built in.
 If you’re planning to start a mental health app, the first useful question is which combination of these categories you want to ship, and how clinical you’re willing to go. Say your goal is to create an app to help reduce anxiety and depression: almost every category below can carry it, from a light mental fitness app to a full clinical product. The calculus shifts for mental disorder apps built around specific mental health conditions: a depression app, an anger management tool, or support for bipolar disorder, obsessive compulsive disorder (OCD), post traumatic stress disorder, or attention problems.
If you’re planning to start a mental health app, the first useful question is which combination of these categories you want to ship, and how clinical you’re willing to go. Say your goal is to create an app to help reduce anxiety and depression: almost every category below can carry it, from a light mental fitness app to a full clinical product. The calculus shifts for mental disorder apps built around specific mental health conditions: a depression app, an anger management tool, or support for bipolar disorder, obsessive compulsive disorder (OCD), post traumatic stress disorder, or attention problems.
The narrower and more acute the condition, the higher the evidence bar. Eating disorder apps and tools for other serious mental health illnesses sit at the top of that ladder; for these mental conditions, the safest pattern is clinician-in-the-loop from day one. Self-management and meditation are the lowest-regulation entry points; teletherapy and crisis intervention sit at the highest end. Build cost and the evidence bar both scale with that choice.
Most of these categories push every serious build into custom mobile applications development once clinical workflows and compliance enter the picture.
| Type | Regulatory load | Evidence bar | Example apps |
|---|---|---|---|
| Self-management | Low; wellness territory until data routes to a clinician, then HIPAA applies | Usability and acceptability studies; trials only among the leaders | Daylio, Sanvello |
| CBT apps | High scrutiny; sits next to digital therapeutics, and DTx claims pull in FDA | The hardest bar: clear lineage to evidence plus guardrails for active suicidality | MindShift CBT, Wysa, Bloom |
| Mindfulness and meditation | Low; the classic wellness entry point | Already cleared: meta-analyses support acute anxiety and depression relief | Headspace, Calm, Insight Timer |
| Peer support | Moderate; moderation and crisis-escalation duties outrank engagement features | Acceptability evidence, thin outcome data | 7 Cups, Wisdo |
| Mental health education | Low; psychoeducation with no care delivery | Implementation feedback, with occasional RCTs | MindPublic, Baby Comfort Guide |
| Crisis intervention | High; reliability is a liability question, and 988 wiring is expected | Uneven; independent evaluations more than trials | Stay Alive, MY3, Suicide Safe |
| Teletherapy | Highest; full HIPAA stack plus therapist licensure across states | Payer-grade outcomes and measurement-based care are table stakes | Talkspace, BetterHelp, SonderMind |
Self-management apps are easy to build and hard to make clinically useful
Self-management apps are the daily driver of digital mental health, overlapping with the consumer shelf of mental wellness apps and self improvement apps: mood trackers, journaling diaries, and habit builders aimed at everyday stress management. They let users log moods and activities, then surface the mood patterns, mood swings, and triggers worth acting on. Done well, that builds real self-awareness and healthier thinking patterns over time. Daylio is the category prototype, backed by usability and acceptability studies.
Founders want to build this first, usually as a pretty chart, but the harder build is data a clinician can use, and the serious version is developing a mental health symptom tracker app that captures PHQ-9 and GAD-7 assessments, sleep, energy, and medication adherence, then routes it to whoever owns the user’s care.
On evidence, Sanvello layers CBT content with randomized and naturalistic trials for anxiety and depression, while Breeze pairs mood tracking with CBT-flavored courses but leans on expert design and user feedback over formal trials.
The phone side is the easy half. Self-tracking earns its keep at the other end: a PHQ-9 trend drifting from 12 to 16 fires a worsening alert, and the clinician can message or schedule a check-in before the next session.
Related: How to Build a Chatbot
Cognitive behavioral therapy (CBT) apps sit closest to digital therapeutics, so they get scrutinized hardest
CBT apps turn what used to live in a workbook or a 50-minute session into structured, evidence-based therapy techniques on a phone: thought records, exposure ladders, worry time, and problem-solving skills training for stress and anxiety, tied to specific problems like panic attacks and insomnia. For founders these sit closer to digital therapeutics than to wellness apps, so clinicians and payers scrutinize them hardest, and the 2026 bar is clear lineage to evidence plus real guardrails for active suicidality.
A CBT app that’s just a worksheet with push notifications won’t clear it. MindShift CBT (Anxiety Canada) is CBT-based self-help for anxiety management with trials showing reduced anxiety and depression over 4 to 16 weeks; Wysa has RCTs across depression, anxiety, and chronic pain plus work on AI-coach therapeutic alliance; Bloom is a self-guided “video CBT” app with traction but limited trials so far.

A thought record runs three repeatable steps: capture the automatic thought, name the distortion behind it, then write the reframe. Structuring those three is most of what separates a CBT app from a worksheet with push notifications.
Mindfulness and meditation apps already cleared the basic evidence bar
Mindfulness and meditation apps are the gateway drug of digital mental health: low-friction and low-stigma, often the first mental health tool otherwise healthy people put on their home screen. They lean on short guided meditations and breathing exercises to reduce stress and anxiety, plus sleep stories and evening practices to improve sleep.
Bigger meditation applications keep folding in adjacent wellness content too: yoga workouts, diet and balanced-meals guidance, even light meal planner features. Streaks keep people coming back long enough to build a meditation habit.
The research here is past “does this work?”: meta-analyses show meditation apps acutely cut depression and anxiety, and Headspace alone has randomized studies on stress, depression, and work outcomes. The open questions now are dose, content, and audience. Calm has RCTs on sleep and mood among adults with sleep disturbance, and Insight Timer pairs a big free library with strong engagement and observational data.

You may also be interested: How to Make a Meditation App Like Headspace
Peer support apps rise or fall on moderation and crisis-escalation rules
Peer support apps sit between therapy and social media: moderated communities, anonymous support groups, and lived-experience forums for people who’ve been through the same thing. The category matters most for teens and young adults, who are hardest to reach through clinics and often working through bullying, heartbreak, or low self confidence. It also fits conditions like chronic pain and addiction, where standard care leaves people in day-to-day isolation.
Scale matters less than founders think, because you’re hosting vulnerable people talking to vulnerable people, so peer support moderation and crisis-escalation rules outrank engagement features. 7 Cups pairs anonymous support groups with volunteer listeners (acceptability evidence, thin outcomes); Wisdo runs guided peer groups for loneliness with strong engagement but no large RCTs; HeyPeers offers certified peer-support meetings built on standardized, evidence-backed models.
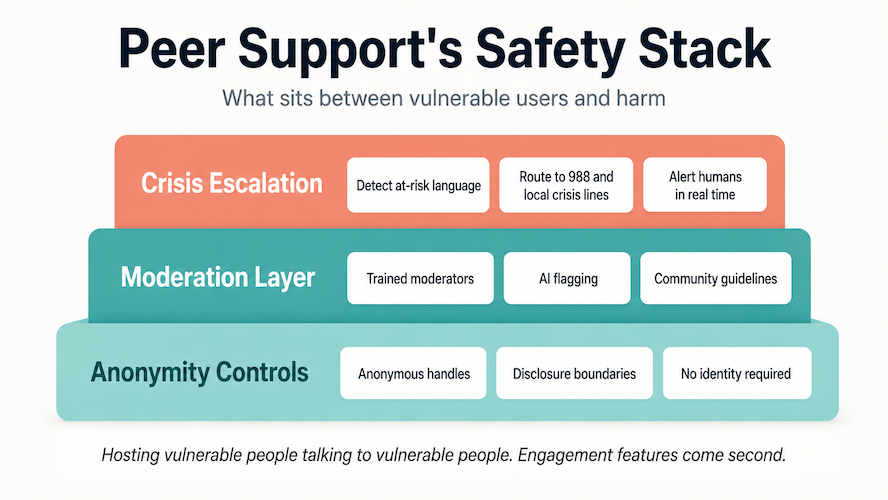
Three layers sit between vulnerable users and harm: anonymity controls at the base (anonymous handles, disclosure boundaries, no identity required), a moderation layer above it (trained moderators, AI flagging, community guidelines), and crisis escalation on top (detect at-risk language, route to 988 and local crisis lines, alert humans in real time).
Mental health education apps lift literacy and cut stigma before the first session
Mental health education apps are asynchronous psychoeducation with better UX: structured content, short videos, interactive diagrams, and self-checks covering common mental health disorders, for everyone from patients and parents to whole workforces of adults. They matter because most people hit Google before a clinician, and health systems, schools, and employers want vetted content to roll out widely; a good one lifts mental health literacy and cuts stigma, so users arrive at a first session already knowing which therapies are on the table.
MindPublic offers open-access literacy for teens and adults; Baby Comfort Guide is an RCT-backed guide for parents of 0 to 24-month-olds, with strong implementation feedback; and the UN’s MindCompanion brings literacy and self-assessment to peacekeepers.
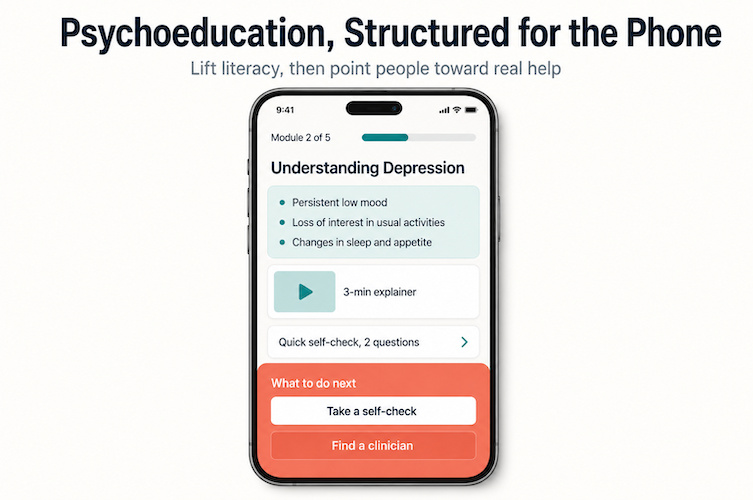
Literacy is the setup, not the payoff. A module earns its place when it ends in a next step: take a self-check, or find a clinician.
For crisis intervention apps, latency and reliability are the whole product
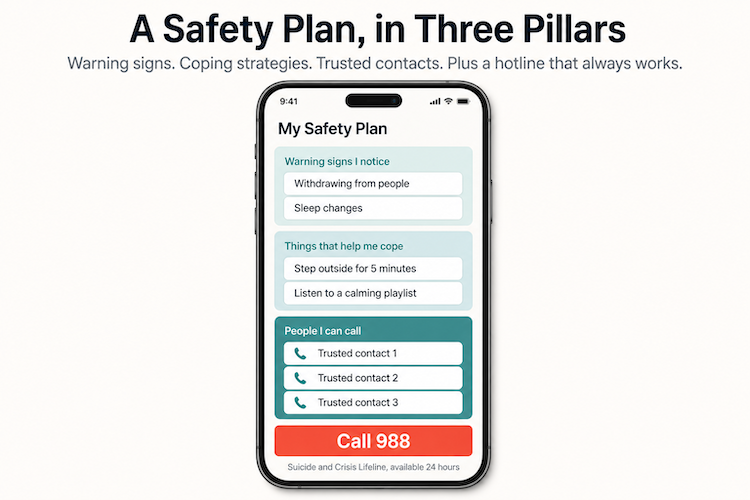
Crisis intervention apps live at the sharp end of digital mental health, built for the worst few minutes of someone’s week: suicidal ideation, a history of suicide attempts, or a panic attack that won’t break. The core is personalized safety plans (warning signs, coping strategies, support contacts), tap-to-call access to crisis lines like 988, region-aware resources, and guidance for supporters and clinicians; for founders the metrics are latency to a working contact and reliability when the path fails, and the liability follows from there.
If you’re designing a mental health app with crisis features, never ship a shiny UI on top of an unreliable safety net. The evidence is uneven: Stay Alive (Grassroots Suicide Prevention, UK) has independent evaluations where 76% of at-risk users said it helped them stay safe; MY3 centers on evidence-backed safety planning with limited app-specific trials; Suicide Safe turns SAMHSA’s SAFE-T assessment protocol into a clinician decision-support tool.
Teletherapy applications compete with brick-and-mortar clinics, so clinical depth is the edge
Teletherapy apps are where a mental health app starts competing with brick-and-mortar clinics: licensed therapists wrapped in scheduling, messaging, billing, and clinical documentation, spanning synchronous video sessions, chat-first therapy and psychiatry, therapist marketplaces, and blended care with medication management.
What matters in a teletherapy platform is whether it handles licensure across 50 states, supports multi-state care without becoming a compliance grenade, and proves better outcomes than a phone number on a clinic website. Many platforms on best telemedicine apps lists already bundle mental health services, so your edge has to come from deeper clinical workflows or a sharper niche, especially since telemedicine app development cost starts in six figures before clinical operations. If you’re creating an app for mental health here, the table stakes are measurement-based care, between-session homework, clear referral paths, and outcome reporting to payers.
The leaders: Talkspace runs large-scale text and live therapy and psychiatry with employer deals and solid data on depression and anxiety symptoms; BetterHelp is the big direct-to-consumer online therapy marketplace, strong on satisfaction if lighter on RCTs; SonderMind matches patients to in-network therapists with measurement-based care and payer outcome reporting.

Related: Telemedicine App Development: Everything You Need to Know
Most serious products blend at least two of these. The “type” you pick determines your regulatory overhead, clinical staffing model, and payer story more than your UI design ever will.
Mental health app compliance and privacy requirements decide what you’re allowed to ship
Compliance work is product work in mental health. Mental health data sits at the top of the sensitivity scale, and regulators treat it that way. The enforcement examples are recent and expensive. Anyone learning how to develop a mental health app in 2026 inherits a patchwork of regulatory guidelines that decide where health data can live, who can see it, and what the app is allowed to call itself. Make treatment claims and you’re in software-as-a-medical-device territory, where FDA clearance becomes part of the roadmap.
HIPAA, GDPR, and regional rules
HIPAA compliance is the floor whenever protected health information and a provider or payer (or their vendors) are involved: signed BAAs with every service that touches PHI, encrypted data storage and transit, access logging, and breach notification.
The bar is rising. HHS has proposed the first major Security Rule update since 2013, and it would turn multi-factor authentication and encryption from “addressable” options into required controls, with 72-hour incident reporting on top. As of July 2026 the proposal (a January 2025 NPRM) has not been finalized: OCR’s spring 2026 target came and went, and OMB’s Unified Agenda now points to July 2027 for final action. [reviewed: July 2026]
Here’s the part founders miss: a direct-to-consumer wellness app with no provider in the loop usually sits outside HIPAA entirely. The FTC covers that gap with Section 5 and the Health Breach Notification Rule, and it has used both. BetterHelp paid $7.8 million in 2023 for routing intake-questionnaire answers to Facebook and Snapchat ad tools after promising privacy. The data privacy rules below stack rather than replace each other, so map your build against each one:
| Rule | Who it catches | What it demands |
|---|---|---|
| HIPAA (US) | Apps handling PHI for providers, payers, or their vendors | Being HIPAA compliant means BAAs, encryption, audit trails, and breach notification; a stricter Security Rule with mandatory MFA and encryption is proposed but not final (OMB now targets July 2027) |
| FTC Act + Health Breach Notification Rule (US) | Consumer health apps HIPAA doesn’t reach | No health data to ad platforms without express consent, plus breach notification; BetterHelp’s $7.8M settlement is the cautionary tale |
| 42 CFR Part 2 (US) | Apps touching substance-use treatment records from Part 2 programs | Consent rules tighter than HIPAA for disclosure; the updated rule’s compliance date landed in February 2026 |
| GDPR / UK GDPR | Any app with EU or UK users | Mental health data is special-category data under Article 9: explicit consent and data minimization, plus a real right to erasure |
| State privacy laws | Consumer health data, state by state (Washington’s My Health My Data, California’s CPRA, others) | Consent for collection and sharing, deletion rights; some states add a private right of action |
| State AI-therapy laws | Apps with AI in the care loop (Utah, Nevada, Illinois, California, Texas, with more states copying the text) | Disclosure that users are talking to AI, licensed oversight or outright bans on AI-delivered therapy (Illinois fines run to $10,000 per violation), crisis-detection duties, and safeguards for minors |
If the matrix feels heavy, the practical move is to classify your data and your claims first, then let that classification pick your stack and your vendors.
| New in 2025 and 2026: state law now regulates AI in mental health apps. Illinois’ WOPR Act bans AI-delivered therapy unless a licensed professional stays in charge, with fines up to $10,000 per violation. Nevada bars AI from presenting itself as professional mental or behavioral health care, while Utah went the disclosure route: chatbots must say they’re software. California and New York added disclosure and crisis-referral duties for companion chatbots; Texas folded chatbot disclosure into TRAIGA. Copycat bills are moving in Florida, Massachusetts, New Hampshire, Ohio, Pennsylvania, and Virginia, and a December 2025 federal executive order kicked off a preemption fight over the whole stack. If AI sits anywhere in your care loop, plan a state-by-state legal review before launch. |
Related: HIPAA Compliant App Development: The Ultimate Guide
Consent, access control, and crisis safeguards
Users hand a mental health app deeply personal information, often in their worst week, so consent has to be legible: what app data is collected, who sees it, what leaves the app, and how to revoke it, in language a stressed person can parse in under a minute. Granular toggles beat one all-or-nothing checkbox, and ad pixels stay out of clinical screens entirely. Anything involving minors needs age gating plus the youth safeguards state laws now spell out.
Inside the app, access control is the daily defense, and these security measures are the minimum:
- role-based permissions that keep a coach from seeing what only the treating clinician should
- multi-factor authentication on anything staff-facing
- biometric login (fingerprint or Face ID) and similar low-friction authentication techniques for users
- audit logs that record who viewed which record when
Data protection starts with encrypting user data at rest and in transit and keeping analytics pipelines blind to PHI; retention windows matter too, because data you no longer hold stops being your liability.
Crisis safeguards round out the layer. Tell users plainly that the app isn’t an emergency service, and put working hotline access in front of them anyway: 988 in the US, local equivalents elsewhere, one tap away, with an optional alert to a trusted contact. Promise nothing you can’t staff, since “24/7 emergency chat” in marketing copy becomes a commitment the moment someone relies on it. And with AI in the loop, crisis detection and escalation logging moved from good practice to statute in some states, so build the hooks now.
With the regulatory floor in place, on to the features worth building on top of it.
Must-have mental health app features (and why you shouldn’t build all 7 in v1)
The right feature set turns a generic product into a mental wellness app that people actually use, and that clinicians can trust. The 7 features below are the building blocks of mental wellness app development, worth thinking through early when you’re designing a mental health app.
Skip too many and you ship a journal with a streak counter; try to build all 7 in v1 and you ship in 14 months instead of 6. Our engineering lead has a shorter version of that warning: “Every 6-month build we’ve watched become a 14-month build broke the same way: compliance and the clinician-facing side got scheduled for later. Later is where mental health timelines double.”
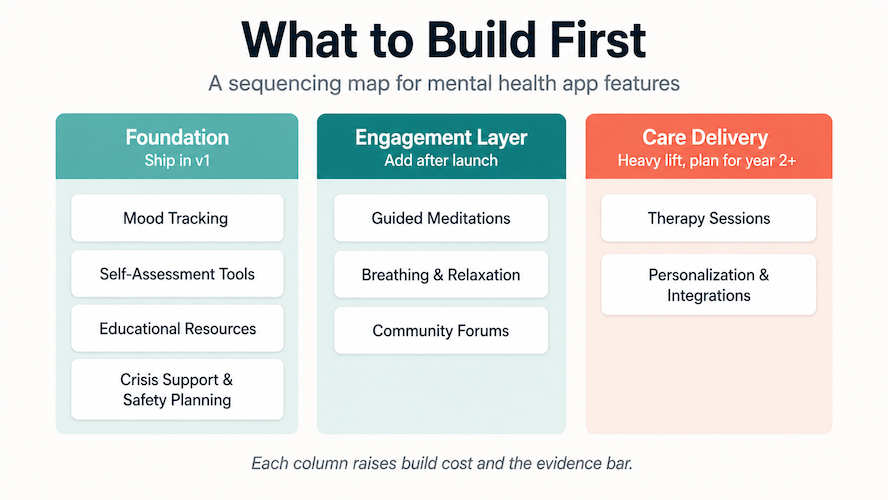
Sequencing beats scope. Ship the foundation in v1 (mood tracking, self-assessment, educational resources, crisis and safety planning), add the engagement layer after launch (guided meditations, breathing, community), and treat therapy sessions and deep integrations as a year-2 lift. Each tier up raises build cost and the evidence bar.
Mood tracking only works when logging is invisible
Mood tracking is still the backbone of mental health management in most consumer-facing builds: quick emotional check-ins for daily mood monitoring, trigger checkers and simple context tags, mood journals for longer notes on thoughts, feelings, and the triggers behind them, and charts that help users track mental health over weeks rather than days. If you’re setting out to develop an app to track mental health, this is the layer to nail first.
The trick with mental health tracking features is to make logging nearly invisible and surface insights in a clean dashboard that filters real patterns from ordinary mood ups and downs; if you want to go deeper on the visualization layer, check out how to build a dashboard web app and apply those principles to symptom and behavior data recording.
Self-assessment tools make the app useful from session one
Self-assessment tools make your app feel useful from the first session by giving users a quick sense of “where am I today?”. A good self-assessment app blends clinically recognized assessment tests (starting with the standard PHQ-9 GAD-7 pair) with conversational interfaces, then turn repeat check-ins into progress tracking a clinician can use between visits. Repeat scores also help users see the depression-anxiety overlap, where symptoms blur together.
For a deeper technical dive into this space, start with our Machine Learning App Development Guide.
Therapy sessions live or die on friction
If you’re serious about teletherapy, the bar is a stable, low-friction virtual therapy experience that doesn’t feel like a bad Zoom clone: patients book appointments in a couple of taps, notifications and reminders that handle time zones gracefully, secure messaging, and high-quality video calls for live sessions. On the clinician side, session notes, outcomes data, scheduling, and billing should live in one place, because healthcare providers shouldn’t have to juggle four tabs to get through an hour of patient work. Any mental health app project that ignores this ships into a non-adopting market.
For extending support beyond the session, see our take on Medical Chatbots: The Future of The Healthcare Industry.
Educational resources should teach escalation as well as coping
Educational resources turn your product into more than a symptom dial by helping people understand the mental health issues they’re dealing with: what a mental health disorder actually is, or why schizophrenia needs a different care path than burnout. Fold in practical modules (text, video, and audio recordings) on sleep hygiene and early relapse warning signs, since knowing when to escalate matters as much as knowing how to cope.
Need inspiration? Our guide on How to Build an Education App shares ways to turn passive content into active learning experiences.
Guided meditations and breathing exercises land harder wired to data
Guided meditations anchor the daily routine around short, repeatable meditation sessions built on proven meditation techniques and well-produced audio content, and they land harder when paired with context like medication reminders or sleep logging. Breathing exercises and other relaxation techniques are tiny interventions with outsized impact once they’re wired to data, timing a practice off sleep patterns or heart rate instead of a fixed morning push.
Even a single well-timed nudge (“breathe before you open email”) can shift perceived stress over a week, and for users who aren’t ready for full sessions, that’s the bridge to deeper engagement, and worth more than bolt-on gamification features.
Community and crisis support are a moderation problem first
Community features connect users who’d otherwise work through this alone, and structured channels (topic channels, small support groups for specific conditions, anonymous posting for sensitive shares) beat an unstructured feed. The build needs serious moderation and clear mental health disclaimers, because you’re hosting vulnerable people talking to vulnerable people.
For higher-acuity populations, add basic emergency support features: safety plans, one-tap 988 hotline integration in the US, and optional emergency messages to a trusted contact, with a visible escalation path to emergency services so the tool in front of someone in distress routes them somewhere safe and fast.
Personalization and integrations are where features compound
The features above compound when they’re stitched together: personalized routines, clinician-configured treatment plans, and integration with a wearable or EHR feeding live data into the loop.
That’s where the app moves from “nice mental health app” to a product that supports care teams, as long as personalization respects the clinical workflow and the user’s limited attention budget. Usable inside a 5-minute session window beats clever.
Integrations that make a mental health app actually useful
A mental health app that lives on an island eventually gets treated like one. The integrations below are what turn a self-contained tracker into part of someone’s actual care: data flowing to the doctors and therapists responsible for treatment, passive signals arriving between visits, sessions that get scheduled and paid for, and conversations that stay private in transit. It’s unglamorous work that shows up in retention and in payer conversations.
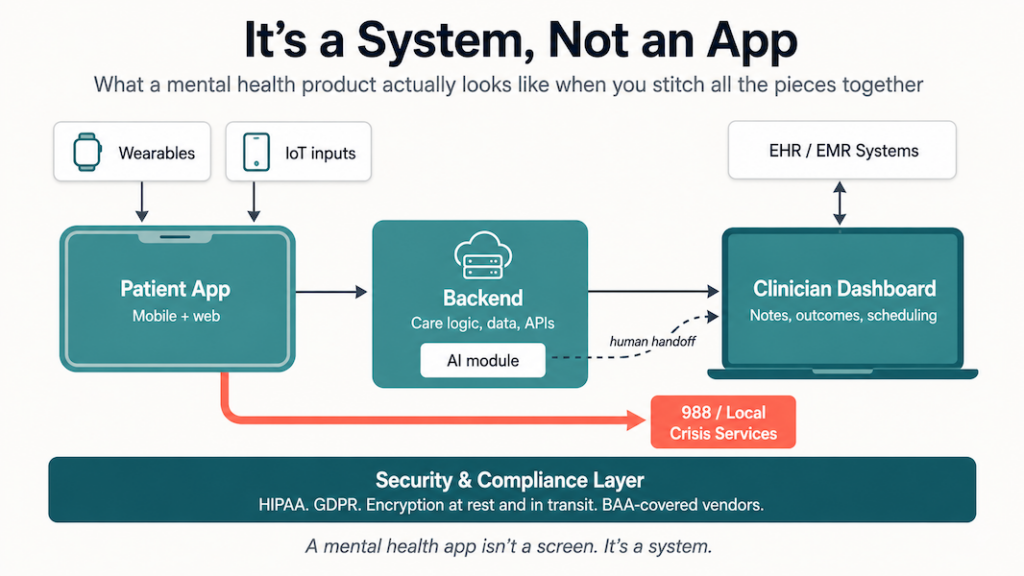
The pieces only pay off wired together: wearable and IoT signals into the patient app, a backend where an AI module escalates to a human, a clinician dashboard synced to the EHR, a crisis path to 988, and a HIPAA and GDPR compliance layer under all of it. A mental health app isn’t a screen. It’s a system.
EHR and EMR integration is where clinician adoption starts
Clinician adoption starts with the chart. When your app writes structured summaries into hospital EHR systems like Epic or Cerner, or at minimum reads the basics from them over FHIR (medications, allergies, recent blood tests), a therapist sees your data inside the workflow they already live in, and the app stops being one more login they ignore. Start EHR integration with read access and clean summaries; full write-back is a bigger lift and worth scoping as its own milestone.
This is also where partnership conversations with payers and integrated care groups begin, because EMR/EHR connectivity is the first thing their technical diligence checks. In therapist app development, where the clinician is the user, the same logic extends to patient lists and shared calendars: meet providers inside the tools they already run their day on.
Related: EMR/EHR System Development Guide
Wearables, sleep data, and remote monitoring inputs catch the drop-off first
Wearables, phones, and consumer sleep trackers give you a real-time view of physical activity, stress levels, and sleep patterns, and a drop-off in either usually shows up days before the patient mentions it in session. That’s the value: passive signals (sleep, steps, heart rate) arriving between check-ins and feeding the whole treatment process, from talk therapy to prescribed medicines, with no extra logging asked of a user who’s already struggling.
Treat any consumer sleep analyzing device and similar tracking tools as context rather than diagnosis, and let Apple Health or Google’s Health Connect handle the device zoo so you’re integrating one rail instead of twelve. Everything in this bucket exists to help providers see the week between sessions, not to impress users with charts.
Also read: IoT App Development Guide
Scheduling, billing, and insurance workflows decide how fast you get paid
Much of app development for therapists comes down to logistics. Appointment scheduling with calendar sync and reminders cuts no-shows, and a health insurance eligibility check before the session prevents the awkward billing conversation after it. Superbills or CPT-coded claims decide whether insurance pays in weeks or in months. If you’re targeting employer or payer distribution, build for their rails early, since EAP referrals and per-member contracts assume your scheduling and billing can talk to their systems.
Secure messaging and video session infrastructure is mostly a buy decision
If you’re in psychological therapy app development, the session layer is the product, and it’s a layer you should mostly buy. HIPAA-compliant audio/video calling SDKs ship with encryption and BAA coverage already handled, which beats rebuilding WebRTC plumbing that adds zero clinical value. Design for the failure path too: an automatic downgrade from a video call to audio saves the session a flaky connection would otherwise end, and asynchronous secure messaging carries the relationship between appointments.
Set message retention to match the rules from the compliance section instead of keeping everything forever by default.
Stitch these four in and the product starts pulling its weight inside a care system, which is where the results in the next section come from.
Creating a mental health app delivers four results you can measure
Creating a mental health app delivers four measurable results: earlier intervention through broader access, lower cost that pulls priced-out users into care, a more personalized experience, and reduced pressure on traditional healthcare systems. Digital tools work alongside traditional therapy as an extension layer, and the outcomes below show up in production metrics like utilization and clinician hours saved.
Better access to mental health support means intervening early
Instant access is the biggest gain: a specialist can support a user without a clinic visit, on the user’s schedule, before an anxiety spike or an early relapse signal escalates into something bigger. Digital entry points also feel safer for people who carry stigma around seeking help, since they can start with an AI bot or a self-help module and bring in human mental health specialists only when needed. That shift gets people into mental health treatment early, when intervention has the biggest effect.
Learn more about artificial intelligence nursing burnout and its role in supporting mental health professionals.
Lower cost compared to face-to-face sessions pulls priced-out users into care
Digital platforms cut the financial barrier that keeps many people out of care: lower session costs at the consumer tier, async and chat-based formats that skip the 50-minute time block, employer-sponsored access to healthcare services through EAP or health-plan rails, and the first reimbursement codes for FDA-cleared digital therapeutics. That price flexibility is why healthcare app development services surged during the pandemic, and digital care still plays the affordable-stopgap role for millions today.
A more personalized care experience is a multi-year moat
Users control their own data (mood history, sleep patterns, medication consistency, symptom curves over months), which is longitudinal patient progress data a periodic office visit never captures. Clinicians come into sessions with that history, which lifts the quality of patient care, and AI-driven micro-interventions adjust exercises, recommendations, and other treatment methods to real-time inputs.
Getting those personalization features to evidence-based status takes a multi-year roadmap, and that’s exactly why they become a moat once you’re there.
Learn about fitness mobile app development in our dedicated blog.
Reduced pressure on traditional healthcare systems frees clinicians for high-acuity work
Tools that help patients self-manage between sessions, reviewing psychoeducation and practicing coping skills on their own time, cut reliance on urgent visits and crisis-level escalations. That frees clinicians for high-acuity cases and reduces operational burden, especially in regions where mental health professionals are scarce.
Trust and tech literacy still need engineering attention, but the core result holds: digital mental health apps absorb volume that clinic-based medicine can’t sustainably handle, and they let the traditional care layer focus on what only humans can do.
Monetization strategies for mental health applications are trust decisions first
Most founders who develop a mental health application start with the same short list of monetization options available for mobile apps, and not all of it fits products built for vulnerable users and regulated care. The job is picking monetization methods that protect clinical value and user trust, beyond whatever your favorite consumer app does.

Two axes sort every model: recurring versus one-time revenue, and whether the user or a third party pays. Subscription and freemium anchor the consumer-scale path; enterprise and payer contracts the clinical-grade one; paid premium and in-app purchases stay niche; ads sit alone in the trust-risk zone. Pricing is flexible. Trust is not.
Subscription and freemium models are the default for a reason
Nearly every top-performing mental health app leans on subscription plans, because the product delivers ongoing support that evolves with the user’s care journey, and the subscription revenue model trades one-off purchases for the predictable ARR investors actually value. Earn it with honest pricing, flexible payment plans, and easy cancellation, plus a clear reason to keep paying past month three, like new programs or clinician touchpoints.
A freemium app is the defensible way in: a free tier that genuinely helps, plus a paid layer that adds depth, with the line usually drawn where live humans and longitudinal data enter the picture.
In-app purchases and paid premium access let users buy at their own pace
In-app purchases are underused in mental health: structured programs and premium content bundles on top of a solid free baseline (the “social anxiety pack” pattern) let users buy modules as they progress without committing to a subscription; seasonal discounts and limited-time app offers can nudge the fence-sitters without cheapening the clinical core.
A one-time paid app still works for tightly scoped tools like a specialist assessment or a clinician utility, with the trade-off that you cap lifetime value on day one. Either way, nudge serious buyers toward web checkout to keep the app stores’ 30% and stay in control of invoicing and refunds.
Enterprise and payer contracts pay slower and retain longer
For clinical-grade products, the real money sits with employers, health plans, and health systems: PMPM (per-member-per-month) contracts and bundled pricing around outcomes like lower PHQ-9 scores, often wired into existing care-management or EAP programs. The path takes longer to validate, and it pays back in higher user retention and tighter coupling to clinical outcomes.
Advertising with caution, and far from anything clinical
You can run a mental health app on advertisements, but the margin for error is near zero: full-screen advertising banners anywhere near crisis content destroy trust and invite App Store review trouble. If sponsors appear at all, keep them to low-key spots in clearly non-clinical areas, and firewall anything touching diagnoses, prescriptions, insurance, or crisis flags from ad targeting completely.
Whichever mix you pick, the throughline holds: in mental health, a monetization model only works if users, clinicians, regulators, and the app stores still trust you in a year. Pricing is flexible; trust is not.
The key aspects of mental health app development get decided before the Gantt chart
Before you commit to sprints and Gantt charts, map out what makes a mental health app actually work: clinical fit and emotional UX come before the commercial model that pays for them. Below is the starter kit by build phase, focused on the parts founders skip most often when learning how to build a mental health app.

Research and planning start with why people quit
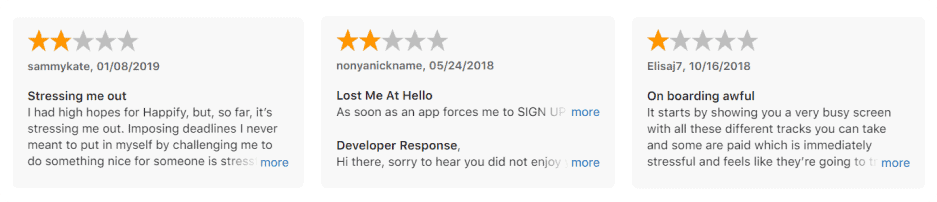
Teenagers with social anxiety and veterans coping with PTSD bring wildly different expectations, so narrow your scope before creating a mental health application and validate user needs through 1:1 interviews, competitor research, and competitors’ 1-star reviews, plus the killer question of why people quit the app they have now.
Proper competitor analysis shows which customer needs the market already serves badly, and where your aims should differ. Get clinical advisors involved early, or you risk a glorified to-do list with a meditation sticker slapped on it. Think past user payments too (employer EAPs, payer partnerships, CPT-coded reimbursement), and never hide help behind a checkout screen mid-crisis.
Design and user experience should assume distress
Design for distress: users may be one tap from closing the app forever, so build user-friendly screens around clarity and calm, from muted palettes to layouts that hold up in dark mode and high-contrast accessibility settings. Localize content and diversify visuals so the app feels inclusive, and skip gamification unless it serves a therapeutic goal; interactive check-ins and short reflection prompts land harder than a “level-up” badge here.
Core features work best built around one job
Pick one core job (supporting recovery, say, or 24/7 therapist access) and build around it: one core feature that works beats ten that kinda do. Mood tracking, AI chatbots, journaling whiteboards, and social features can all wait their turn.
Development and security favor cross-platform builds and vendor BAAs
Cross-platform frameworks are usually the fastest route to market, with Python services behind them if AI is in the picture; the full trade-offs live in the tech stack section below. Compliance is the non-negotiable layer covered earlier, so here’s the short version: encrypt everything and bake in access controls from day one, and Firebase and Airtable don’t belong anywhere near anything remotely clinical. Better yet, work with vendors who offer signed BAAs and compliance out of the box.
Testing and deployment treat confusion as a harm signal
Ship fast, but don’t break trust: beyond functional testing, this category calls for usability testing with neurodiverse users, clinical review of content and flow, data privacy audits, and pre-launch penetration testing of any AI components. If users report confusion or hesitation, treat it as a harm signal, because mental health users notice friction differently than productivity-app users do.
Post-launch maintenance runs on a quarterly clock
Mental health content and clinical practices evolve, and the app has to keep up: quarterly releases and rotating therapeutic content are baseline for the category, with vulnerability testing running on its own ongoing clock.
Once people rely on your product for their emotional wellbeing, every feature you ship (or break) carries higher stakes than a typical consumer software product. Treat your backlog like a care plan.
Step-by-step guide on how to create a mental health app, one decision per step
Here’s how to make a mental health app step by step: each of the five steps in the development process has a real decision attached, and skipping one makes the next harder. The sequence assumes you’re an entrepreneur planning to start a mental help app from scratch, not bolting features onto an existing clinical product.
Step 1: Choose the target audience and platforms
Whether you’re aiming at seniors or teenagers shapes your platform mix, so pin down the patient cohort first: the age group you’re helping (teen, adult, senior), what competitors have taught your audience to expect, whether you’re building for a specific community (LGBTQ users, veterans, new parents) whose trust bar is higher, and a typical patient profile. Ideally, a few participants from your target audience stick around for the next step and help narrow the UX/UI of the solution.
Step 2: List possible features and run rapid prototyping
When it comes to custom developing an app, listing features and testing them in a prototype verifies design ideas before you spend on code, which cuts cost by an order of magnitude and shortens how long it takes to build your app.
Validating the business idea (and the business plan behind it) with zero coding is where entrepreneurs save the most, because coding is the most expensive part of mental health software development. Bring developers in at this stage too; they’ll flag the designs that look fine in Figma and break in implementation.

Step 3: Develop the app
This is where most of the product development time goes, and we recommend Agile with interim tests every iteration, building both sides from the start: the patient app and the clinician surface behind it. Keep the timeline honest with off-the-shelf components (HIPAA-compliant video SDKs, chat with audio messages) and a DevOps pipeline that’s ready before sprint one, with cybersecurity best practices per HIPAA regulations throughout.
At Topflight Apps, we lower the tech barrier (and the cost with it) by reusing a library of ready-made modules for authentication, appointment scheduling, chat, and secure messaging, the prerequisites common to most mental health applications.
Read our guide on how to find and hire mobile app developers
Step 4: Test the app
Testing runs through every iteration, but this step is the big pre-release sweep: functional and performance passes, compatibility testing, interface testing, plus unit, stress, and security testing at minimum. Give the security and interface passes the most attention: unpatched security vulnerabilities and confusing screens are where mental health apps lose user trust first.
Related: Mobile App Testing: Methods, Best Practices, Tools and More
Step 5: Release and keep updating
Once testing clears, the app heads through app store submission (fewer tremors if you’re working with pros), ideally with a mobile marketing campaign behind it. Then comes post-launch mode: track in-app analytics, address user requests, and ship updates on a steady rhythm, with a clean DevOps setup keeping maintenance costs from creeping.
Engagement data from the live app will drive the next round of updates and point to growth areas research didn’t show you.
Working through these steps gives you a real path to a mental health applications development project that holds up in the market.
The tech stack for mental health apps is downstream of three decisions
The tech stack decisions that actually matter are platform reach, on-device ML or AR/VR needs, and how many systems you’ll integrate with (EHR, CRM, payments, video). Most modern stacks can carry a mental health application development project once those three are picked, because framework choice is downstream.
Mobile app technologies default to cross-platform
React Native or Flutter cover iOS and Android from one codebase and extend to web later with shared logic, which is why cross-platform is the default for most mental health MVPs. Native mobile technologies, e.g. Swift for iOS and Kotlin for Android earn their keep when you need top-tier UX or platform capabilities like on-device machine learning, AR/VR, or OS-level biometrics.
On either path, security comes from the libraries and managed services you wire in (encryption, KMS, BAA-covered hosting), so don’t let anyone tell you the framework itself carries it.
Backend and infrastructure follow the workload
Node.js with TypeScript as the app server on a managed cloud like AWS or GCP is the solid default for chat-heavy, real-time workloads like teletherapy sessions. Go Python (FastAPI or Django) when AI and data science sit at the center, and keep CPU-heavy model work on dedicated workers off the main API. Either way, provision with IaC and stick to HIPAA-eligible service tiers, since one misconfigured bucket undoes everything the compliance section set up.
Databases and security foundations keep PHI and analytics apart
Managed PostgreSQL or MySQL plus Redis for caching covers most builds, with pgvector joining the stack if you’re adding retrieval for an AI layer. Data security here is mostly discipline: store PHI only in encrypted, BAA-covered instances and keep analytics data physically separate from it; design for right-to-erasure and export from day one, because retrofitting both at your first enterprise deal hurts.
Integrations and communication tools belong behind middleware
The integrations section above covers why EHR and billing connections matter; at the stack level the job is wiring them so a vendor outage or a leaky API never touches PHI. The short rule is to put middleware between you and every external system instead of scattering direct calls through the codebase. And if a system you depend on has no usable API, budget for building one, because that’s a real line item.
Analytics and monitoring run blind to PHI
Product analytics (Mixpanel or Amplitude) tells you where users churn, while OpenTelemetry and a SIEM cover the engineering and security sides of the same story. The hard rule for data analytics in this category: PHI stays out of event streams by design, and the flows you watch most closely are the high-risk ones, assessments and crisis paths first.
A sample architecture of a mental health app, layer by layer
Most builds in this category assemble the same blocks: cross-platform clients, a real-time backend, an encrypted data layer, and a ring of integrations with an AI service alongside. The table maps each technology stack layer to the options we reach for and the mental health-specific notes that usually surface by week three of an engagement.
| Layer | Recommended option(s) | When to prefer it | Key trade-offs | Mental health-specific notes |
|---|---|---|---|---|
| Client app (mobile) | React Native (with Expo) or Flutter (cross-platform) |
|
|
|
| Client app (mobile) | Swift + SwiftUI (iOS) / Kotlin + Jetpack Compose (Android) |
|
|
|
| Web client | React / Next.js, Angular, or Vue |
|
|
|
| Backend (API + business logic) | Node.js (TypeScript) on AWS / GCP / Azure |
|
|
|
| Backend (API + business logic) | Python (FastAPI / Django) with ML services |
|
|
|
| AI / LLM layer | BAA-covered model endpoints (Azure OpenAI, AWS Bedrock, Google Vertex AI) + RAG over a vector store (pgvector, Azure AI Search) |
|
|
|
| Database | PostgreSQL or MySQL (managed), plus Redis for caching and pgvector for RAG |
|
|
|
| Infrastructure & DevOps | AWS / GCP / Azure with IaC (Terraform, CloudFormation) |
|
|
|
| Integrations | EHR/EMR (FHIR / HL7), CRM, Payments, Video SDKs |
|
|
|
| Analytics & Observability | Mixpanel/Amplitude + OpenTelemetry + SIEM |
|
|
|
10 takeaways from negative reviews on mental health apps (we’ve read them so you don’t have to)
Learning how to create a mental health app that doesn’t earn one-star reviews starts with reading the one-star reviews. We’ve watched the same 10 complaints surface in mental health app reviews for years. The patterns below are the ones worth designing around.
The one-line version: the fastest ways to earn a one-star review in this category are a broken login, a pushy paywall, cold design, and content that never refreshes, and every one of them is visible in competitors’ reviews before you write a line of code.
- Test every login path end to end. Facebook, Google, and Apple sign-in can each break in subtle ways that show up first in one-star reviews.
- Make every UX element earn its place. If users can’t tell why they earn points, they stop chasing them within a week.
- Find the balance between upselling a subscription and giving value first. The reviews you don’t want all sound the same: tricked into paying.
- Design has to signal safety. A mental health app that looks clinical-cold or commercial-pushy turns people away in equal measure.
- Onboarding decides whether you get a second session. Every extra screen between download and first useful moment adds frustration and costs users.
- Keep security from getting in the way of ordinary use. A 2FA flow that locks people out at the wrong moment ends in uninstall.
- Be clear about pricing, renewal terms, and how to cancel. Back it up with support that responds same-day and an in-app knowledge base that answers the questions reviews keep raising.
- Triage every reported issue by impact on the therapeutic loop. A crash mid-journal entry costs you more than a layout glitch.
- Support the latest mobile OS and the screen sizes your patients actually use.
- Ship new content on a rhythm. Long-time users notice when the same exercises keep cycling, and user engagement drops.
Every one of the 10 is cheaper to design around than to apologize for in a review reply.
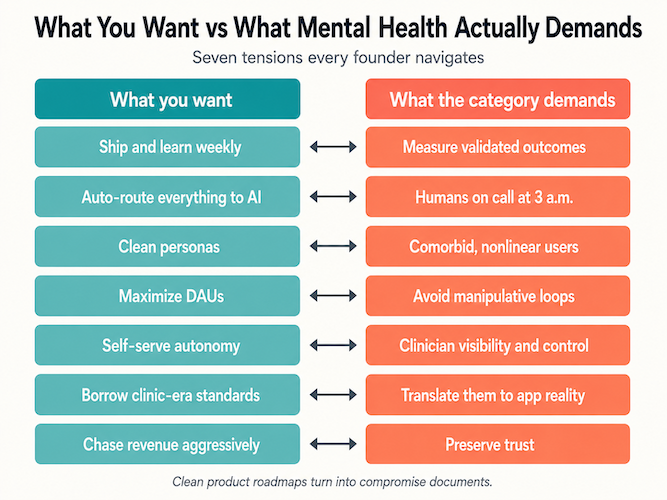
The key challenges in mental health app development sit between the what and the how
The hard part of making a mental health app is everything between the what and the how: the messy constraints that turn clean roadmaps into compromise documents. By this point you know what to build and roughly how. Below are the friction points we hit on most mental health app development projects, in the order they tend to bite, each with the move that actually mitigates it.
Clinical validation and product credibility
Everyone says “be evidence-based,” and few teams have a playbook for what that means with 18 months of runway and a half-built app. Clinicians, payers, and outside experts want validated instruments, product wants to ship weekly, and users just want something that helps them sleep, which leaves you somewhere between a university lab and vibes-based care.
The mitigation: pick a small outcome set (PHQ-9 or GAD-7 paired with retention) and design features so they can be evaluated in the wild; modest benefit in a real population beats an RCT on a toy feature.
Safety, crisis escalation, and risk management
Once crisis features exist, you own the what-if moments: disorder aggravation triggered by the wrong content, a user typing explicit suicidal intent at 3:12 a.m., or the app opened in a country where your hotline list is outdated. The ToS line “we are not an emergency service” is the easy part; the hard part is making the UX and backend do what the ToS claims.
The mitigation: design three coordinated routes (technical flags and audit trails, an operational on-call definition of “urgent,” and legal language that matches reality), then test that a 3:12 a.m. flag actually reaches a human before sunrise.
Engagement and long-term retention
The apps with the strongest scientific foundations often lose on day-to-day engagement, and the consumer fixes (guilt-trip streaks and FOMO mechanics) would look terrible on the front page of a newspaper. Real users compound the problem by behaving nothing like personas: motivation fluctuates week to week, and clinical-sterile copy amplifies the very stigma you’re trying to dissolve.
The mitigation: habit loops with the manipulative bits stripped out, plus paths that tolerate a missed week without making someone feel they’ve failed the app, in copy that works for the barely-holding-it-together user as well as the stable one.
Balancing self-guided support with professional care
The promise of a mental health app is autonomy; the hard part is knowing when to take it back. A milder mental health issue can be safe to support fully app-driven, while others need a mental health professional in the loop, and the handoff to human support has to feel like care rather than a sales funnel (“you seem worse, upgrade to Pro therapy!” is the temptation to resist).
The mitigation: define escalation criteria clinically instead of commercially, and keep expectations honest, because a CBT bot pitched as an alternative to trauma work lands too clinical for casual users and too casual for clinicians, and neither audience commits.
Regulatory and operational complexity
The compliance section mapped the rules; the deeper problem is that most mental health standards were written for clinical settings, before app-based care existed as a category. What does informed consent mean when the first interaction is a 20-second onboarding carousel, and which framework do you anchor to (CBT or stepped care) when you’re not a licensed provider yourself?
The mitigation: stitch clinical guidelines, digital-health regulatory expectations, app-store policies, and your internal ethics bar into one stack coherent enough for your medical advisors and your PM, with legal annotating throughout.
Building a sustainable business without losing trust
You’re shipping the app and building the company around it at once: raising in a market that already burned through several mental-health hype cycles, and negotiating B2B2C deals without turning users into engagement metrics in someone else’s slide deck. The mitigation: let the monetization principles from earlier do the work (value first, no surprise paywalls) and treat investor updates like clinical claims, provable or unsaid.
Every monetization decision (subscriptions, ads, enterprise contracts, B2B distribution) feeds back into the thing that keeps a mental health product alive: trust. You can refactor a tech stack. Trust with patients and clinicians takes much longer to rebuild than to lose.
Mental health app development cost starts around $70,000 and climbs with scope
The cost of developing a mental health app varies with scope, app type, platform count, and integration depth: a simple mood tracker with self-monitoring features starts around $70,000, while a teletherapy app starts closer to $140,000, and both are figures for the MVP version you build on from there. If you’ve already researched telemedicine app development cost, expect serious mental-health builds to land in a similar band, with extra budget going into safety workflows, clinical integrations, and audit-ready data handling. And when you build a mental illness app, make sure quotes cover the back end (database plus an admin area for content management), since owners forget the parts that don’t show up in the demo.
Founders keep asking what HIPAA itself adds to mental health app development cost. Most agencies quote a 20 to 35% premium; we plan the funds in dollars instead: $5,000 to $25,000 of compliance work on an MVP (risk analysis, BAAs, encryption, baseline policies), climbing to $40,000 to $100,000 once you’re selling to organizations that ask for pentest reports and vendor due diligence.
| Scenario / app type | What the MVP typically includes | Platforms | Backend & admin scope | Typical MVP cost range (USD) | When this makes sense |
|---|---|---|---|---|---|
| Simple mood tracking app |
|
|
|
~ $70,000 (lean MVP starting point) |
|
| Self-management / CBT tools app |
|
|
|
~ $90,000 – $140,000 |
|
| Teletherapy app (video + messaging) |
|
|
|
Starts around ~ $140,000 (grows with multi-region and complex features) |
|
| Crisis support / safety-plan app |
|
|
|
~ $100,000 – $160,000 |
|
| Blended-care platform (therapy + programs + analytics) |
|
|
|
~ $200,000 – $350,000+ (depending on integrations and scale) |
|
| Hidden cost drivers (all types) |
|
||||
Related articles: Understanding App Development Costs, Healthcare App Development Costs
The future of mental health app development looks like infrastructure
The next decade of mental health apps comes down to whether your product behaves like infrastructure: clinically credible and evidence-backed enough to sit inside real care pathways without spooking regulators.
From standalone apps to care infrastructure
The market growth from the overview section runs through specific channels: teletherapy as a standard employer and payer benefit, digital therapeutics like Sleepio clearing NICE/FDA-style validation into reimbursement, and health systems and mental health practices wiring apps into intake and stepped-care workflows with real budget behind them.
Future winners look like services that slot into payer and provider stacks, with APIs and real-world evidence behind the placement and governance documents ready for procurement review.
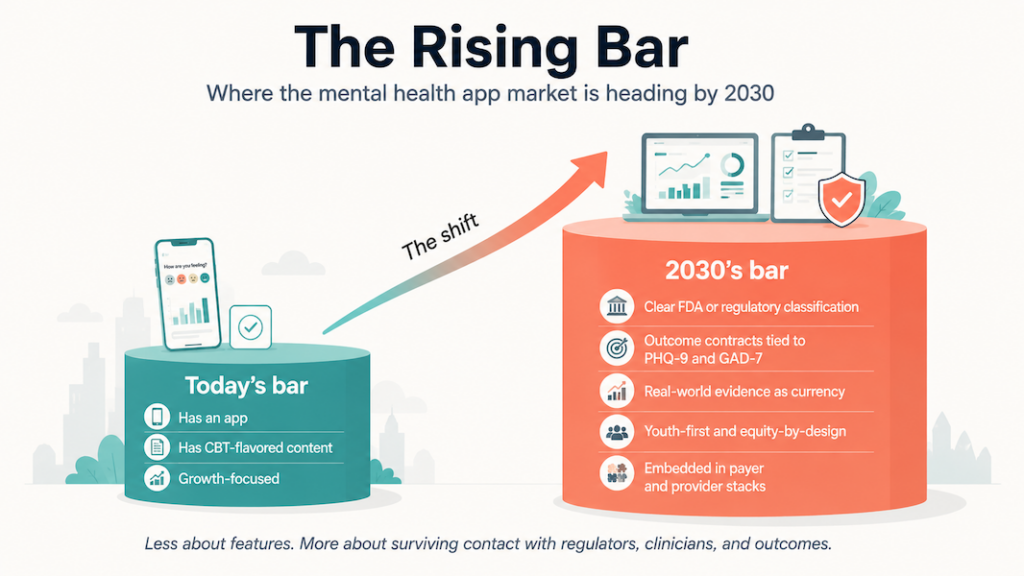
Today’s bar clears with an app, some CBT content, and a growth chart. By 2030 the bar is FDA classification, outcome contracts tied to PHQ-9 and GAD-7, real-world evidence, equity by design, and a slot inside payer and provider stacks. Less about features, more about surviving contact with regulators, clinicians, and outcomes.
Safer and more regulated use of AI, or a category assigned the hard way
The easy era of “just add a chatbot” is ending, with FDA’s Digital Health Advisory Committee examining generative AI in mental-health software and the state laws from the compliance section multiplying. We’ve seen AI engines recommend a glass of bourbon to relax, which is why you can’t train healthcare machine learning algorithms on live patients and why every model needs a clean human handoff at the edge of its depth.
The bar for AI mental health app development now is provably safe AI scoped to its true regulatory category (wellness bot, clinical decision support, or medical device), with logged behavior and audit trails that survive an OCR review, and marketing language that matches, or you’ll get assigned a category the hard way.
Stronger focus on evidence and outcomes, with payment attached
Investors learned the “growth without outcomes” lesson the expensive way, so expect insurer-grade requirements for real-world evidence and outcome contracts where PHQ-9 or GAD-7 reductions drive payment, plus tighter scrutiny of safety data like adverse events and escalation performance. The products that hold up are built as if a clinical trial were already booked: clean measures and clear cohorts from day one, with instrumentation that can answer “does this actually help?” next to the usage analytics.
Greater attention to youth, access, and equity, now in the spec
WHO now frames youth mental health in terms of digital determinants: how platforms and feeds shape risk and resilience, and how apps either compound or buffer those forces. That pushes youth-first safety and consent flows (built for under-25s with heavy social media exposure) and equity as a spec requirement (from language to device constraints) to the front of mental health app design. The bar is rising from “not obviously harmful” to “demonstrably helpful, especially for vulnerable groups.”
The future of mental health app development is surviving contact with regulators and clinicians, with real-world outcomes data as the arbiter, while still shipping something people want to use. For founders, developing a mental health application will increasingly mean proving safety and measurable outcomes, with equity in the spec from day one, on top of the usual product-market fit story.
Topflight Apps’ experience with mental health app development, in four shipped products
We’ve seen upfront planning make or break mental health application development in practice, especially once real clinicians and patients start using the product. Topflight Apps’ experience in mental health app development covers several projects in the space; as a mental health app development company, we’ll walk through the four that show the range.
| Product | The problem | What we built | The result |
|---|---|---|---|
| Xzevn | Users needed a low-friction way to build emotional self-awareness, with the treatment team watching from outside | A chatbot diary and content recommendation engine, plus an admin web app for the care team | The client landed a spot in a business incubator. Case study. |
| Soberbuddy | An inherited build, overcomplicated by unneeded ML, that the client couldn’t monetize | A CBT-based recovery chatbot with mind-body relapse prevention, rebuilt on a simpler stack | Funding reached $1.25 million, retention up 300%, rating from 3 to 4.5, customer-acquisition cost cut in half. Case study. |
| Mi-Life | Caregivers were expected to memorize 1,300+ pages of client-specific protocols | A HIPAA-compliant RAG assistant (GPT-4o, Azure AI Search, Whisper) answering by voice or text without exposing PHI | Fewer medication errors, faster onboarding, higher staff satisfaction, and a backend built to replicate across group homes. Case study. |
| Respirosa | Making breathwork a habit users keep | A breathwork app synced to the user’s own Spotify picks, with tempo-locked visual guidance | A consumer wellness build that crosses into care-program territory. Case study. |
Xzevn
Xzevn is a content recommendation engine and chatbot diary for emotional health that tracks mood changes day to day: users log emotions in conversation and react to recommended articles and quotes, building self-awareness and steadier mental health habits around time management, goal setting, and self-improvement, with no attempt at diagnosis. The treatment team sees those interactions through a connected admin web application.

Soberbuddy
Soberbuddy is a chatbot guiding people through addiction recovery (alcohol and drugs) with evidence-based relapse prevention for drinking and drug triggers: cognitive behavioral therapy plus mind-body relaxation techniques.
We inherited the build from a team that had overcomplicated it with unnecessary machine learning blocks and couldn’t help the client monetize; since Topflight Apps took over, funding has reached $1.25 million, retention is up 300%, the app store rating climbed from 3 to 4.5, and the cost of acquisition dropped by half.

The Soberbuddy story covers how to start a mental health app grounded in cognitive behavior therapy on the first go, a pattern that repeats across our mental health therapy app development work.
Related Article: Addiction Recovery App Development
Mi-Life: AI assistant for behavioral and developmental health
Mi-Life is the deep end of our mental health application development services: a HIPAA-compliant, RAG-based AI assistant (GPT-4o, Azure AI Search, Whisper) for caregivers, family members, and relatives supporting individuals with developmental disabilities and Autism.
The problem was cognitive overload, with staff expected to memorize over 1,300 pages of client-specific protocols; Mi-Life turns that into real-time answers by voice or text, covering behavior plans, medication details, and emergency steps without exposing PHI during AI processing.

The outcome: fewer medication errors and faster onboarding, with higher staff satisfaction and a multi-tenant backend built to replicate across group homes and behavioral health organizations.
Respirosa
Respirosa is a mindfulness app with a twist: breathwork practiced to the user’s favorite music, with visual cues synced to the beat. Users handle the music selection, picking a tune by mood or artist; the app pulls it from Spotify, and a tempo-locked animation runs the breathing session.
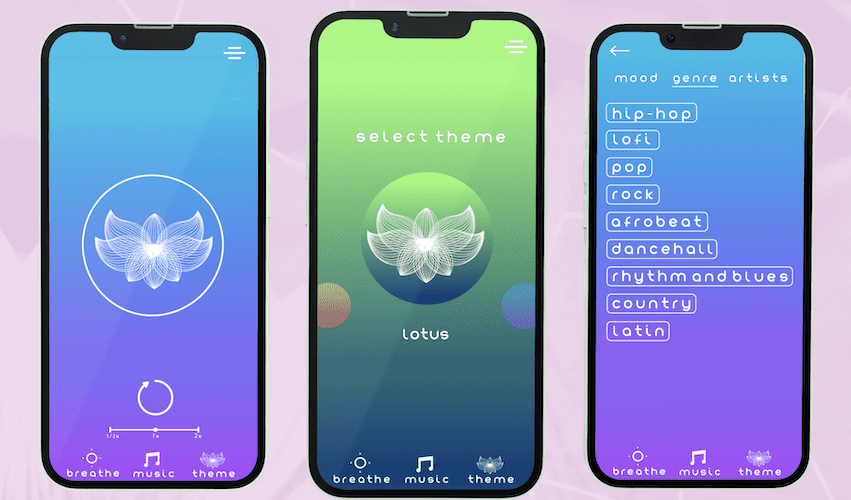
Projects like Respirosa show how wellness app development blurs the line between calm consumer tools and clinically meaningful support, especially when breathing practice and habit loops wire into broader care programs. That crossover is the real test of mental health mobile app development services.
Reach out if you want to develop a mental health app with mental health app developers who’ve already shipped in this category, or you want yours to outperform what’s in the App Store. Our mental health app development services run from a validation-stage MVP to the blended-care platforms at the top of the cost table, the working range of a mental health application development company.
Related articles:
- A Guide to Building a Mental Health Chatbot
- Healthcare App Development Guide
- How to start a healthcare startup
- How to Create a Telehealth App
- How to collect healthcare data for your mobile apps
- Building Healthcare Apps that Improve Patient Data
- Artificial Intelligence in Healthcare
- How to build a doctor appointment app
- Wearable Technology in Healthcare
- Building Healthcare Chatbots
[This blog was originally published in September 2020 and has been updated for more recent data]
Frequently asked questions
How much does it cost to develop a mental health app?
$70,000 to $140,000 for a typical MVP, depending on the build. Bigger blended-care platforms can run $200,000 and up; reach out for a quote, and we’ll map app development solutions to your specifics.
What tools should I consider to build a mental health app that relies on AI?
For an AI-powered mental health app today, look at LLM APIs (GPT-4o, Claude, Gemini), LangChain or LlamaIndex for orchestration, a vector store for RAG (Azure AI Search, Pinecone, or pgvector), and Whisper for voice. PyTorch still earns a spot for custom-trained models. Whatever you pick, route model calls through BAA-covered endpoints if PHI is anywhere near the conversation.
Do I need to provide any certificates to list my mental health solution in app stores?
No certificates as such, though both stores give health apps extra review: expect to declare your data practices (Apple’s privacy labels, Google’s health apps declaration) and to show regulatory clearance if you claim medical-device functionality.
How long does it take to build an average mental health tracker app?
4 to 6 months for a HIPAA-grade MVP. A pure wellness tracker without PHI handling can ship in 3 months, but most mental health apps cross into HIPAA territory fast.
Does my mental health app need to be HIPAA compliant?
If it stores or transmits any protected health information, yes. And if you’re a direct-to-consumer app outside HIPAA’s reach, the FTC’s health-data rules apply instead, so the privacy work doesn’t go away.
How do I build a mental wellness app that's engaging and personal?
Use AI frameworks and a chatbot that learns from discussions with patients, then add the engagement basics: content that rotates on a rhythm and habit loops without the guilt mechanics.
What are mental health apps?
Mental health apps are mobile or web tools that support emotional and psychological wellbeing, from self-management trackers and CBT programs to meditation apps, education apps, peer communities, crisis tools, and teletherapy platforms that connect users with licensed therapists. They range from low-regulation wellness tools to clinical-grade software, and which side of that line you build on decides most of your compliance load and cost.
How is user privacy and data protected?
Through layers: encryption of user data at rest and in transit, multi-factor and biometric authentication, role-based access, and audit logs, all under whichever rules apply to your build (HIPAA, the FTC’s health-data rules, GDPR, and state privacy laws). The practical bar: no health data to ad platforms without express consent, and retention windows with deletion on a schedule.
What are the main types of mental health apps?
Seven: self-management, CBT, mindfulness and meditation, peer support, mental health education, crisis intervention, and teletherapy. Regulation scales across that list, with self-management and meditation at the light end and teletherapy and crisis tools at the heavy end.
Are mental health apps regulated by the FDA?
Only when they claim to treat or diagnose. Wellness and self-management apps stay outside FDA’s scope; digital therapeutics making clinical claims need clearance, and CBT apps sit closest to that line. State AI-therapy laws now add a separate layer on top.
Do AI therapy chatbots have to disclose they are AI?
In a growing list of states, yes. Utah and New York require mental health chatbots to say they’re software, Illinois and Nevada go further and ban AI-delivered therapy without licensed oversight, and California and Texas fold chatbot disclosure into broader AI laws. Build disclosure in by default.
What features should a mental health app include in its MVP?
Pick one core job and build around it: mood tracking with PHQ-9 and GAD-7 self-assessment for a tracker, or scheduling, video, and secure messaging for teletherapy. Crisis escalation paths belong in v1 regardless of type; the other features earn their way in later.
How do mental health apps make money?
Four routes: subscriptions and freemium (the default), in-app purchases, enterprise and payer contracts (slower to close, better retention), and advertising, which stays far from anything clinical. Trust decides which of these your users will tolerate.
How much does HIPAA compliance add to mental health app development cost?
Budget it in dollars: $5,000 to $25,000 of compliance work at the MVP stage (risk analysis, BAAs, encryption, baseline policies), climbing to $40,000 to $100,000 once buyers ask for pentest reports and vendor due diligence. On a typical mental health app development budget, that’s the reality behind the 20 to 35% premium other agencies quote.